

Fasting glucose and body mass index as predictors of activity in breast cancer patients treated with everolimus-exemestane: The EverExt study
- PMID: 28878375
- PMCID: PMC5587713
- DOI: 10.1038/s41598-017-10061-2
Fasting glucose and body mass index as predictors of activity in breast cancer patients treated with everolimus-exemestane: The EverExt study
Abstract
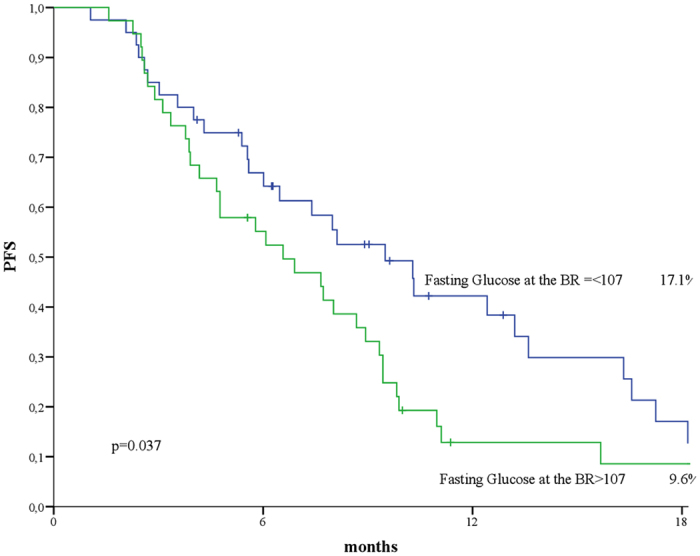
Evidence on everolimus in breast cancer has placed hyperglycemia among the most common high grade adverse events. Anthropometrics and biomarkers of glucose metabolism were investigated in a observational study of 102 postmenopausal, HR + HER2- metastatic breast cancer patients treated with everolimus-exemestane in first and subsequent lines. Best overall response (BR) and clinical benefit rate (CBR) were assessed across subgroups defined upon fasting glucose (FG) and body mass index (BMI). Survival was estimated by Kaplan-Meier method and log-rank test. Survival predictors were tested in Cox models. Median follow up was 12.4 months (1.0-41.0). The overall cohort showed increasing levels of FG and decreasing BMI (p < 0.001). Lower FG fasting glucose at BR was more commonly associated with C/PR or SD compared with PD (p < 0.001). We also observed a somewhat higher BMI associated with better response (p = 0.052). More patients in the lowest FG category achieved clinical benefit compared to the highest (p < 0.001), while no relevant differences emerged for BMI. Fasting glucose at re-assessment was also predictive of PFS (p = 0.037), as confirmed in models including BMI and line of therapy (p = 0.049). Treatment discontinuation was significantly associated with changes in FG (p = 0.014). Further research is warranted to corroborate these findings and clarify the underlying mechanisms.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
