

Unusual Entities of Appendix Mimicking Appendicitis Clinically - Emphasis on Diagnosis and Treatment
- PMID: 28878833
- PMCID: PMC5574067
Unusual Entities of Appendix Mimicking Appendicitis Clinically - Emphasis on Diagnosis and Treatment
Abstract
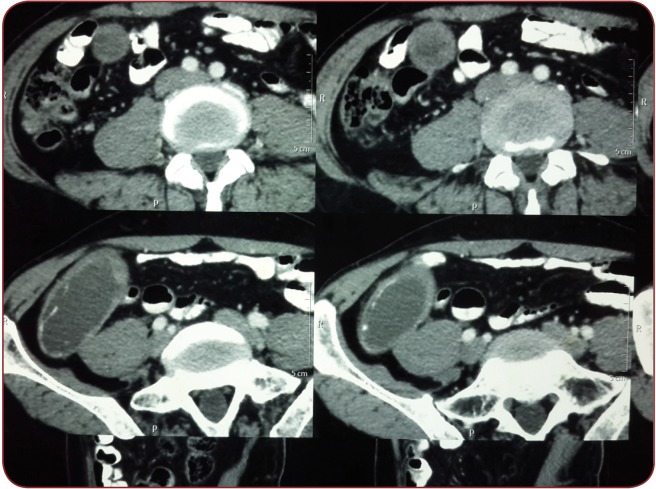
Background: Abdomen is considered a magic box or a Pandora box where you will get different, unexpected pathologies along with rare entities. Appendicitis is the commonest emergency in surgery which presents challenges to surgeons because of a myriad list of differential diagnosis including both medical and gynaecological pathologies. Preoperative imaging plays an important role in diagnosis and management.
Aims and objectives: To study the rare atypical anatomical and surgical presentations of appendix in patients with clinical features of appendicitis. We focus on the clinical features and the role of investigations for the radiological part and management.
Material and methods: This study was done in M.M. Institute of Medical Sciences and Research, Mullana, Ambala, from November 2014 to July 2016. This was a retrospective study. We found 168 cases with the diagnosis of appendicitis, out of which 19 were with rare entities.
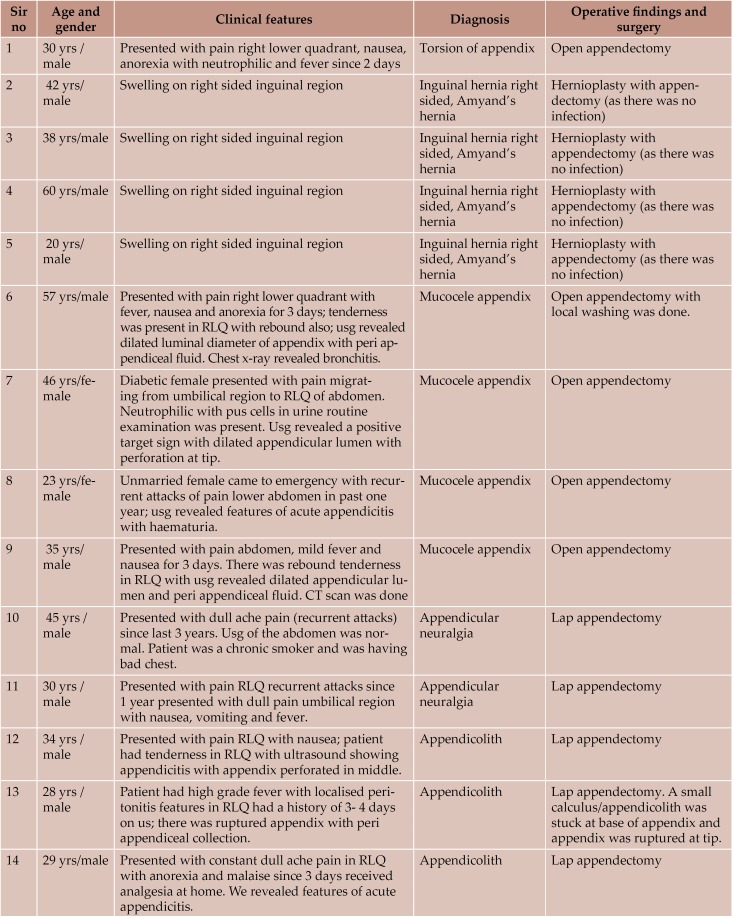
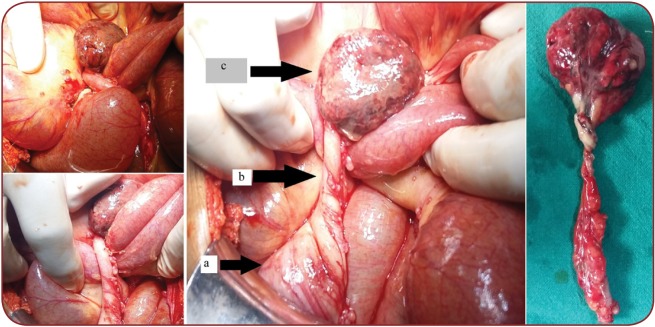
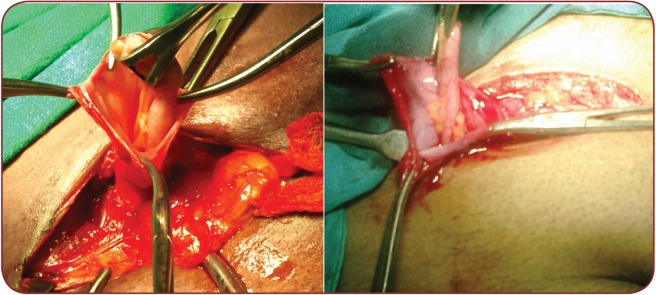
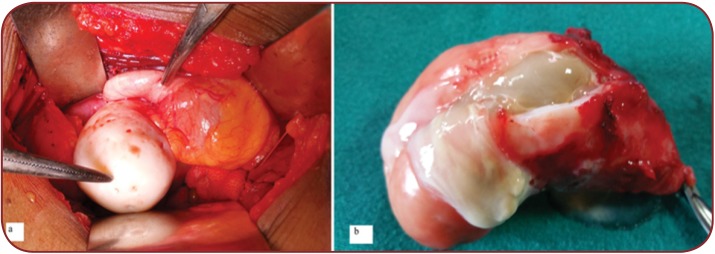
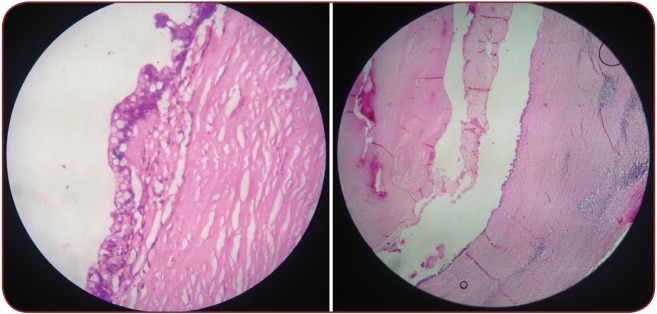
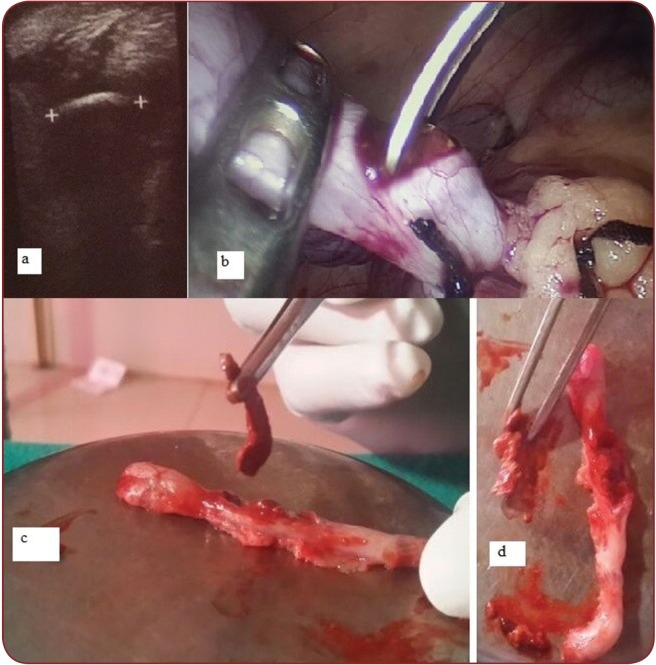
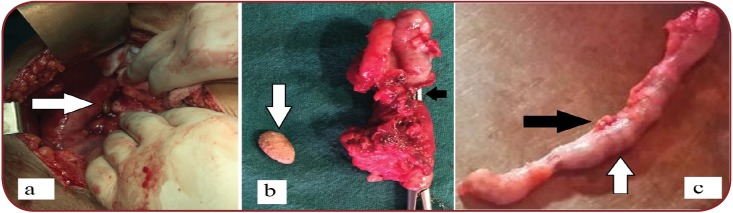
Results: Subjects of both genders were aged between 20 and 60 years. Out of 19, 15 were males and 4 females. Four patients were operated for inguinal hernia but incidentally we found appendix in the hernial sac termed as Amyand's hernia. Another patient presented with obstruction and appendix was forming a band diagnosed as torsion of appendix. Two most interesting cases were diagnosed as appendicular neuralgia and relieved by appendectomy. Out of 19 cases, 7 cases were operated for appendicitis diagnosed as appendicolith. In all the cases appendectomy was done without encountering any complications. Symptom free patients were operated for appendicular neuralgia. No malignancy was found in mucocele appendix at follow up. There were no complications by the 6-month follow-up.
Conclusion: As we came across with different entities of appendix presented with appendicitis, patients should be investigated before proceeding for surgery. In our study, there were incidental findings for which surgeons were not aware of the diagnosis and even for the patient. In inguinal hernia, ultrasonography was not done, diagnosis being made on clinical basis. Clinical and radiological investigations play an important part in early diagnosis and management.
Figures
Similar articles
-
Amyand's hernia in the children: a single center experience.Surgery. 2010 Jan;147(1):140-3. doi: 10.1016/j.surg.2009.09.038. Epub 2009 Nov 11. Surgery. 2010. PMID: 19910011
-
Amyand's hernia: a report of 18 consecutive patients over a 15-year period.Hernia. 2007 Feb;11(1):31-5. doi: 10.1007/s10029-006-0153-8. Epub 2006 Sep 26. Hernia. 2007. PMID: 17001453
-
[Amyand's hernia and complicated appendicitis; case presentation and surgical treatment choice].Cir Cir. 2016 Jan-Feb;84(1):54-7. doi: 10.1016/j.circir.2015.06.012. Epub 2015 Jul 31. Cir Cir. 2016. PMID: 26238589 Spanish.
-
[Amyand's hernia: a report of two cases and review of the bibliography].Cir Cir. 2014 Mar-Apr;82(2):195-9. Cir Cir. 2014. PMID: 25312320 Review. Spanish.
-
A rare case of Amyand's hernia in a 67-year-old male. A case report and review of the literature.Ann Ital Chir. 2015 Jun 24;86(ePub):S2239253X15023907. Ann Ital Chir. 2015. PMID: 26098854 Review.
Cited by
-
Neuroendocrine apendicopathy in morphologically normal appendices of patients with diagnosis of acute appendicitis: Diagnostic study.Ann Med Surg (Lond). 2020 Nov 6;60:344-351. doi: 10.1016/j.amsu.2020.10.044. eCollection 2020 Dec. Ann Med Surg (Lond). 2020. PMID: 33224488 Free PMC article.
-
Mucocele of the appendix presenting as an exacerbated chronic tubo-ovarian abscess: A case report and comprehensive review of the literature.Medicine (Baltimore). 2019 Sep;98(39):e17149. doi: 10.1097/MD.0000000000017149. Medicine (Baltimore). 2019. PMID: 31574819 Free PMC article. Review.
References
-
- Van Rossem CC, Treskes K, Loeza DL, van Geloven AA. - Laparoscopic appendectomy for chronic right lower quadrant abdominal pain. Int J Colorectal Dis. 2014;29:1199–1102. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials