

Phospho-AXL is widely expressed in glioblastoma and associated with significant shorter overall survival
- PMID: 28881571
- PMCID: PMC5584143
- DOI: 10.18632/oncotarget.18468
Phospho-AXL is widely expressed in glioblastoma and associated with significant shorter overall survival
Abstract
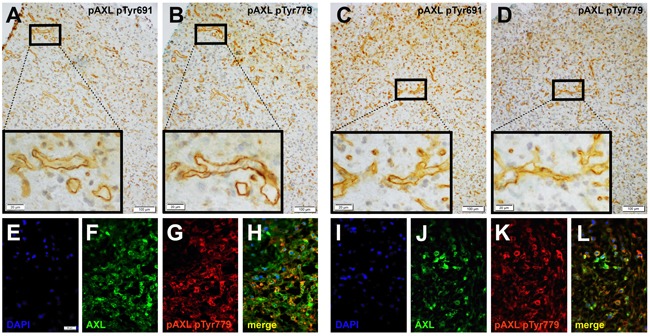
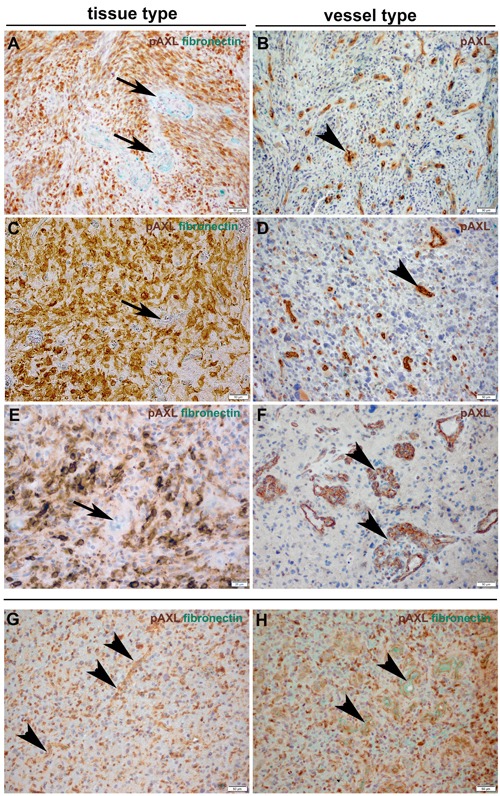
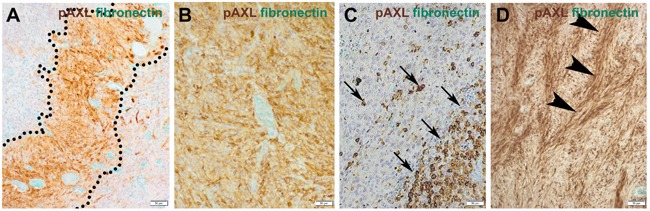
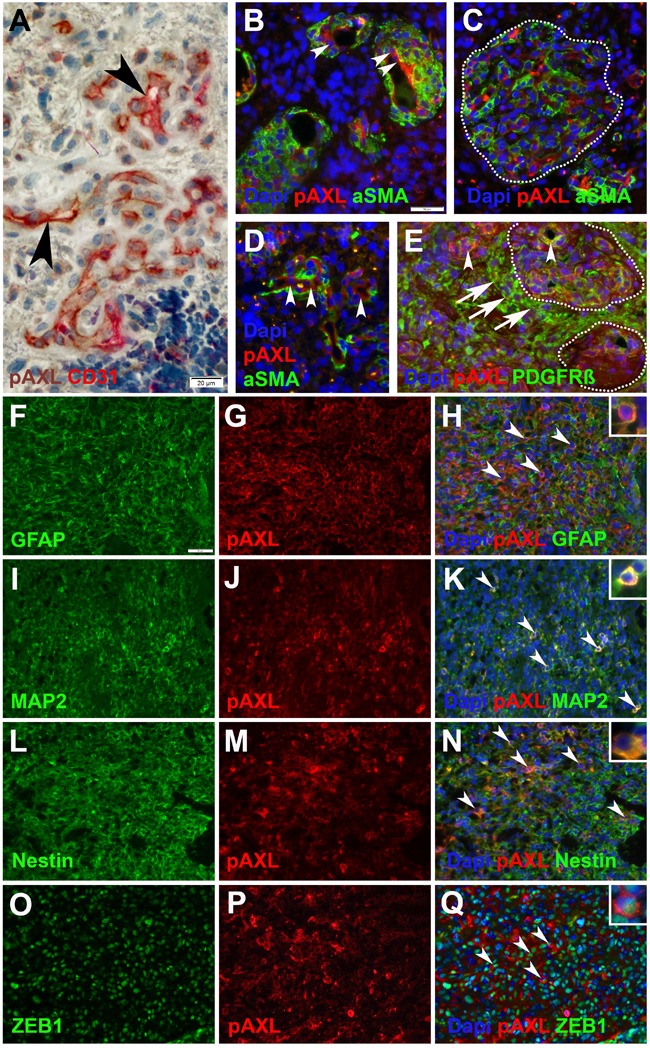
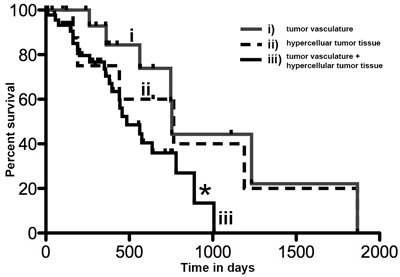
Receptor tyrosine kinase AXL (RTK-AXL) is regarded as a suitable target in glioblastoma (GBM) therapy. Since AXL kinase inhibitors are about to get approval for clinical use, patients with a potential benefit from therapy targeting AXL need to be identified. We therefore assessed the expression pattern of Phospho-AXL (P-AXL), the biologically active form of AXL, in 90 patients with newly diagnosed GBM, which was found to be detectable in 67 patients (corresponding to 74%). We identified three main P-AXL expression patterns: i) exclusively in the tumor vasculature (13%), ii) in areas of hypercellularity (35%), or iii) both, in the tumor vasculature and in hypercellular areas of the tumor tissue (52%). Pattern iii) is associated with significant decrease in overall survival (Hazard ratio 2.349, 95% confidence interval 1.069 to 5.162, *p=0.03). Our data suggest that P-AXL may serve as a therapeutic target in the majority of GBM patients.
Keywords: Pathology Section; glioblastoma multiforme (GBM); glomeroid tufts; overall survival; phospho-Axl (P-AXL); receptor tyrosine kinase AXL (AXL).
Conflict of interest statement
CONFLICTS OF INTEREST No conflicts of interest exists in the submission of the manuscript and the manuscript is approved by all authors for publication.
Figures
References
-
- Ostrom QT, Gittleman H, Fulop J, Liu M, Blanda R, Kromer C, Wolinsky Y, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol. 2015;17(Suppl 4):iv1–iv62. doi: 10.1093/neuonc/nov189. - DOI - PMC - PubMed
-
- Stupp R, Dietrich PY, Ostermann Kraljevic S, Pica A, Maillard I, Maeder P, Meuli R, Janzer R, Pizzolato G, Miralbell R, Porchet F, Regli L, de Tribolet N, et al. Promising survival for patients with newly diagnosed glioblastoma multiforme treated with concomitant radiation plus temozolomide followed by adjuvant temozolomide. J Clin Oncol. 2002;20:1375–82. doi: 10.1200/JCO.2002.20.5.1375. - DOI - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–96. doi: 10.1056/NEJMoa043330. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
