

Institutional maternal and perinatal deaths: a review of 40 low and middle income countries
- PMID: 28882128
- PMCID: PMC5590194
- DOI: 10.1186/s12884-017-1479-1
Institutional maternal and perinatal deaths: a review of 40 low and middle income countries
Abstract
Background: Understanding the magnitude and clinical causes of maternal and perinatal mortality are basic requirements for positive change. Facility-based information offers a contextualized resource for clinical and organizational quality improvement. We describe the magnitude of institutional maternal mortality, causes of death and cause-specific case fatality rates, as well as stillbirth and pre-discharge neonatal death rates.
Methods: This paper draws on secondary data from 40 low and middle income countries that conducted emergency obstetric and newborn care assessments over the last 10 years. We reviewed 6.5 million deliveries, surveyed in 15,411 facilities. Most of the data were extracted from reports and aggregated with excel.
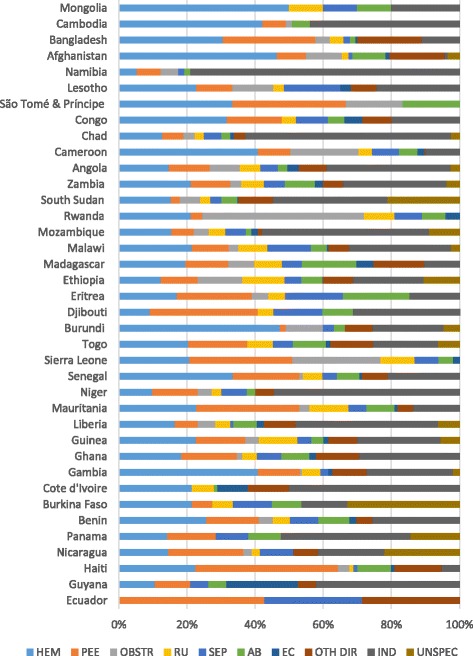
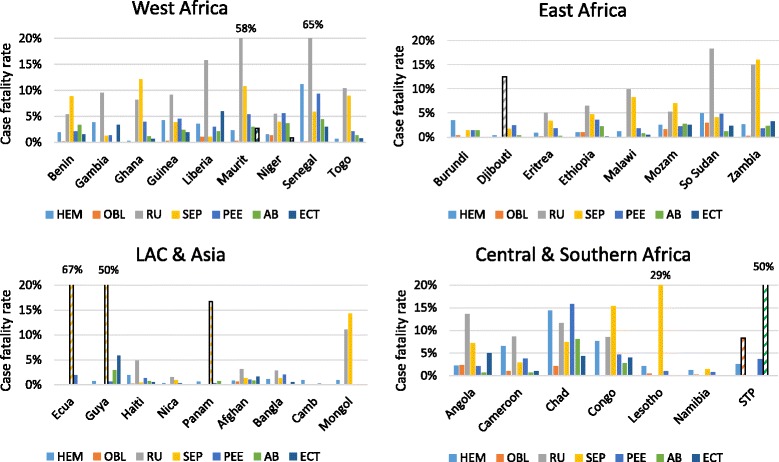
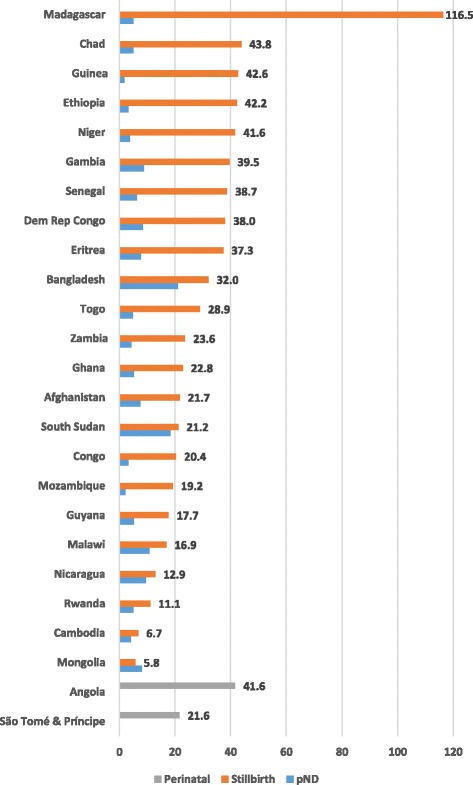
Results: Hemorrhage and hypertensive diseases contributed to about one third of institutional maternal deaths and indirect causes contributed another third (given the overrepresentation of sub-Saharan African countries with large proportions of indirect causes). The most lethal obstetric complication, across all regions, was ruptured uterus, followed by sepsis in Latin America and the Caribbean and sub-Saharan Africa. Stillbirth rates exceeded pre-discharge neonatal death rates in nearly all countries, possibly because women and their newborns were discharged soon after birth.
Conclusions: To a large extent, facility-based findings mirror what population-based systematic reviews have also documented. As coverage of a skilled attendant at birth increases, proportionally more deaths will occur in facilities, making improvements in record-keeping and health management information systems, especially for stillbirths and early neonatal deaths, all the more critical.
Keywords: Cause of maternal death; Cause specific case fatality rate; Direct and indirect deaths; Early neonatal death rate; Perinatal mortality; Stillbirth rate.
Conflict of interest statement
Ethics approval and consent to participate
The authors did not seek approval from an internal review board for this secondary data analysis since the primary sources of the data were reports in the public domain, based on surveys that had already undergone ethical approval. Names of women or other identifying information were never included in primary data collection. Countries followed the guidance of their ministries of health or the research institutions that carried out the surveys, and when required, approval of the protocols and data collection instruments from local institutional review boards was obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organization: Every Newborn: an Action Plan to End Preventable Deaths (ENAP) [http://www.who.int/maternal_child_adolescent/topics/newborn/en/]. Accessed 7 Sept 2017.
-
- World Health Organization: Strategies toward Ending Preventable Maternal Mortality (EPMM) [http://who.int/reproductivehealth/topics/maternal_perinatal/epmm/en/]. Accessed 15 May 2017.
-
- Blencowe H, Cousens S, Jassir FB, Say L, Chou D, Mathers C, Hogan D, Shiekh S, Qureshi ZU, You D, et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health. 2016;4(2):e98–e108. doi: 10.1016/S2214-109X(15)00275-2. - DOI - PubMed
-
- Cousens S, Blencowe H, Stanton C, Chou D, Ahmed S, Steinhardt L, Creanga AA, Tuncalp O, Balsara ZP, Gupta S, et al. National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. Lancet. 2011;377(9774):1319–1330. doi: 10.1016/S0140-6736(10)62310-0. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
