

Disseminated tuberculosis among hospitalised HIV patients in South Africa: a common condition that can be rapidly diagnosed using urine-based assays
- PMID: 28883510
- PMCID: PMC5589905
- DOI: 10.1038/s41598-017-09895-7
Disseminated tuberculosis among hospitalised HIV patients in South Africa: a common condition that can be rapidly diagnosed using urine-based assays
Abstract
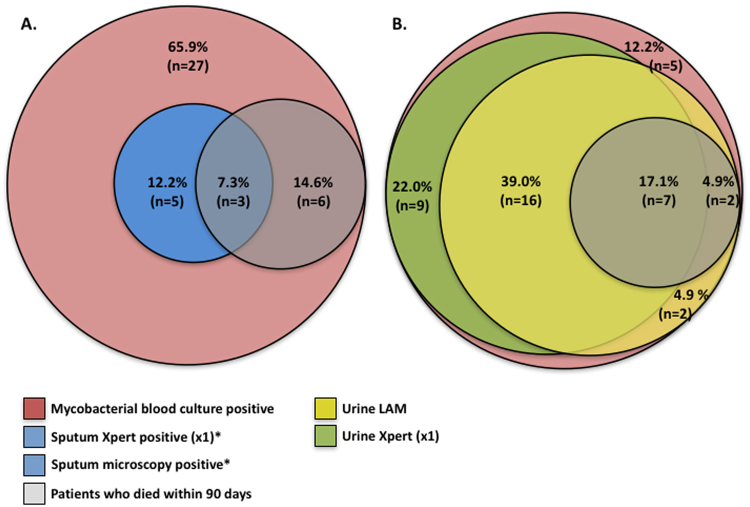
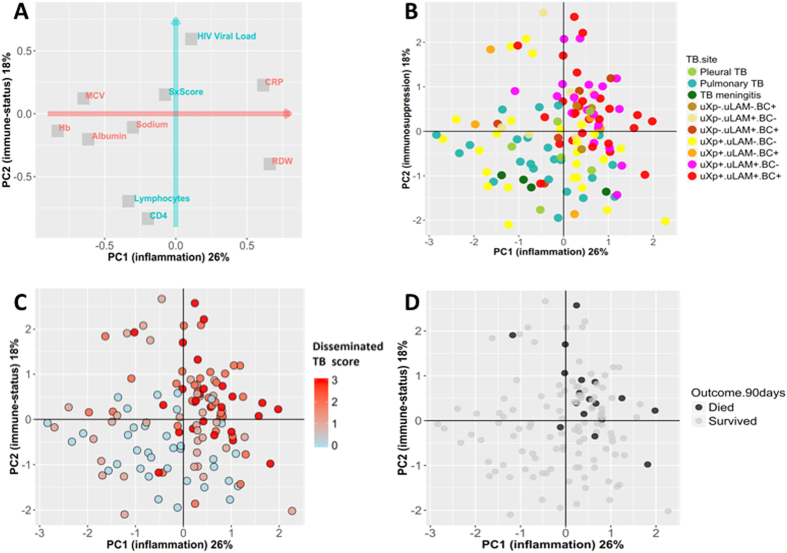
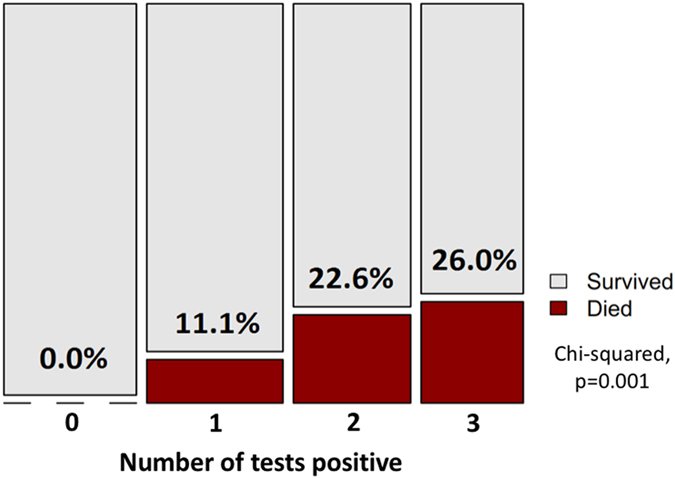
HIV-associated disseminated TB (tuberculosis) has been under-recognised and poorly characterised. Blood culture is the gold-standard diagnostic test, but is expensive, slow, and may under-diagnose TB dissemination. In a cohort of hospitalised HIV patients, we aimed to report the prevalence of TB-blood-culture positivity, performance of rapid diagnostics as diagnostic surrogates, and better characterise the clinical phenotype of disseminated TB. HIV-inpatients were systematically investigated using sputum, urine and blood testing. Overall, 132/410 (32.2%) patients had confirmed TB; 41/132 (31.1%) had a positive TB blood culture, of these 9/41 (22.0%) died within 90-days. In contrast to sputum diagnostics, urine Xpert and urine-lipoarabinomannan (LAM) combined identified 88% of TB blood-culture-positive patients, including 9/9 who died within 90-days. For confirmed-TB patients, half the variation in major clinical variables was captured on two principle components (PCs). Urine Xpert, urine LAM and TB-blood-culture positive patients clustered similarly on these axes, distinctly from patients with localised disease. Total number of positive tests from urine Xpert, urine LAM and MTB-blood-culture correlated with PCs (p < 0.001 for both). PC1&PC2 independently predicted 90-day mortality (ORs 2.6, 95%CI = 1.3-6.4; and 2.4, 95%CI = 1.3-4.5, respectively). Rather than being a non-specific diagnosis, disseminated TB is a distinct, life-threatening condition, which can be diagnosed using rapid urine-based tests, and warrants specific interventional trials.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. Global tuberculosis report 2016 (2016).
-
- UNAIDS. World AIDS Day 2015 - Fact Sheet. 1–8 (2015).
-
- World Health Organization. Global tuberculosis report 2015 (2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
