

Techniques and long-term effects of transjugular intrahepatic portosystemic shunt on liver cirrhosis-related thrombotic total occlusion of main portal vein
- PMID: 28883536
- PMCID: PMC5589901
- DOI: 10.1038/s41598-017-11455-y
Techniques and long-term effects of transjugular intrahepatic portosystemic shunt on liver cirrhosis-related thrombotic total occlusion of main portal vein
Abstract
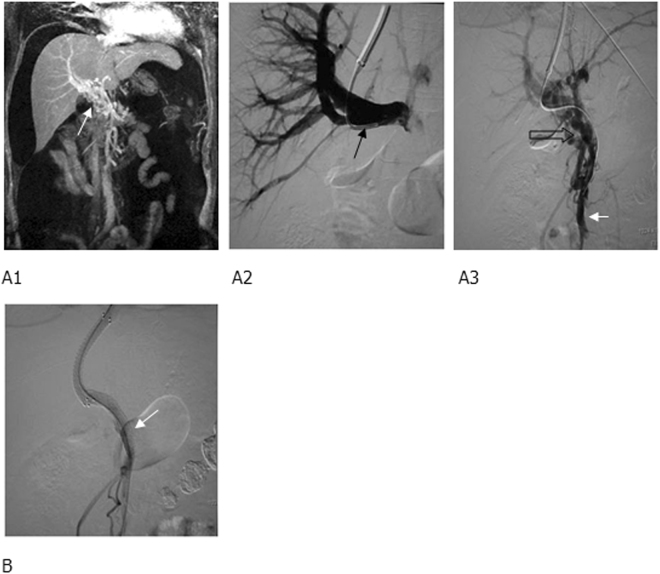
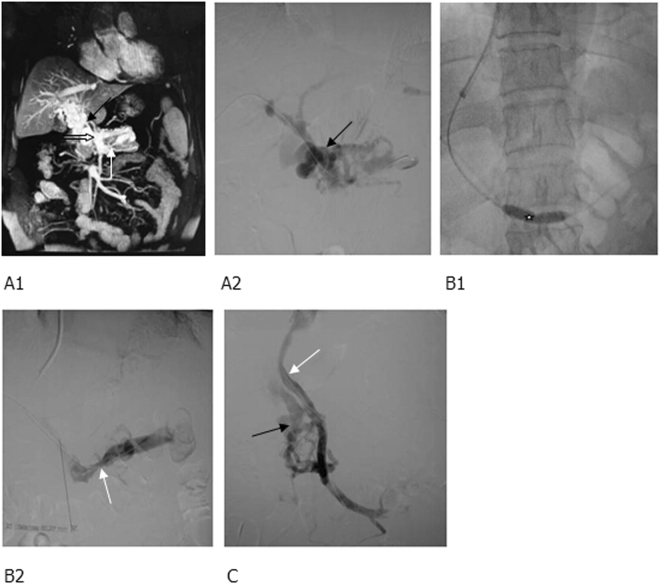
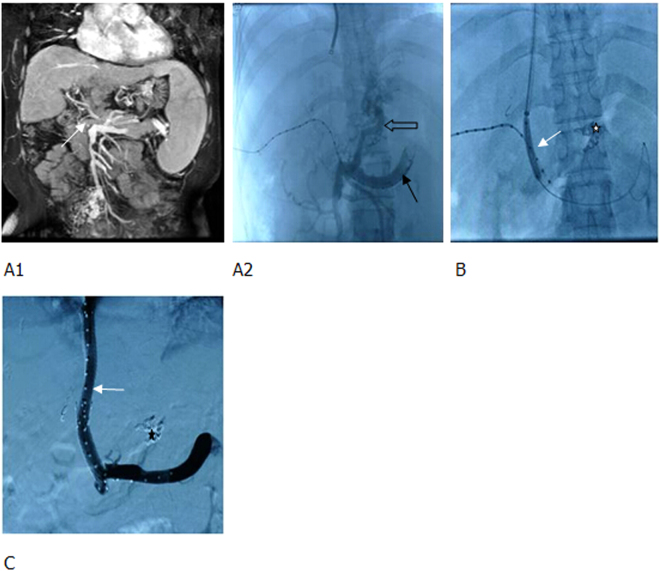
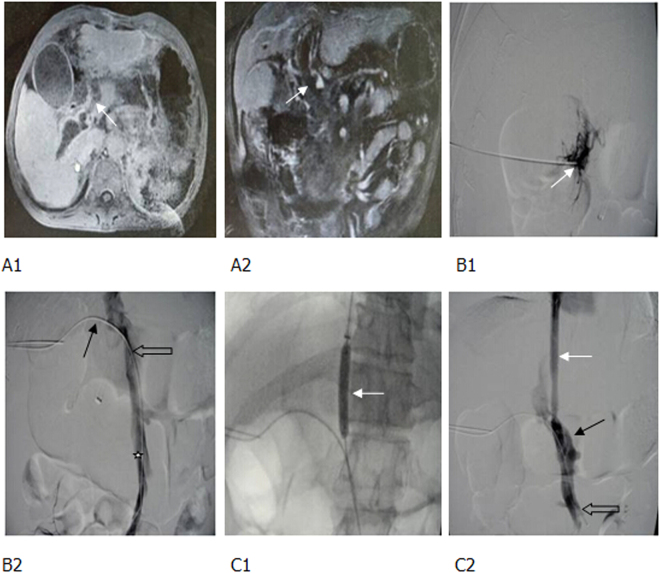
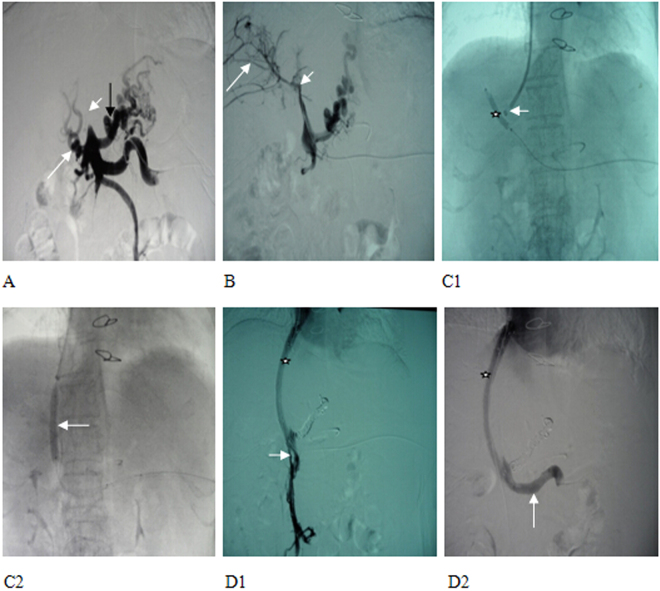
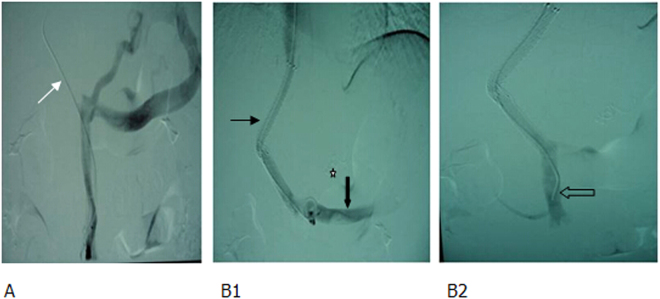
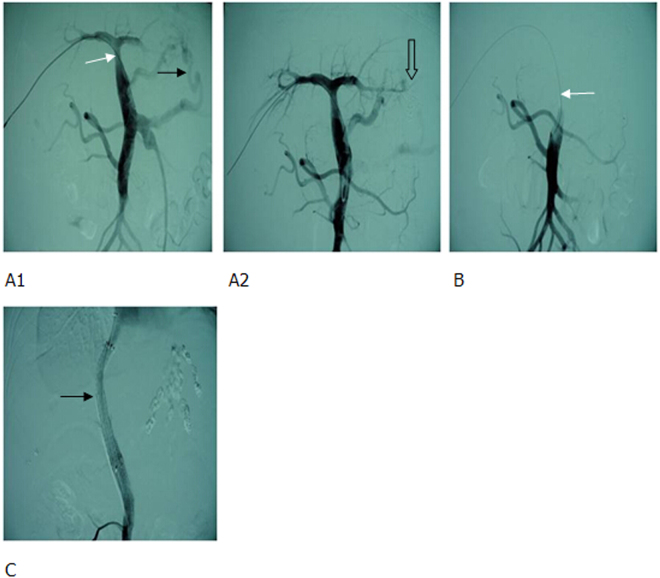
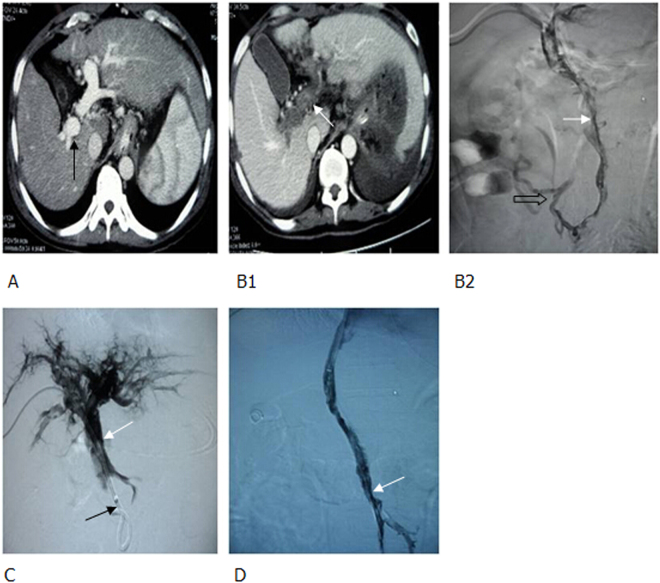
Portal vein hypertension (PVH) in liver cirrhosis complicated with portal venous thrombosis (PVT) has been mainly treated with transjugular intrahepatic portosystemic shunt (TIPS). The clinical effects of TIPS have been confirmed, however, no large-scale studies have been focused on technical analyses and a long-term follow-up, especially on thrombotic total occlusion of main portal vein (MPV). To demonstrate critical techniques and clinical outcome of TIPS on liver cirrhosis-related thrombotic total occlusion of MPV, 98 patients diagnosed with liver cirrhosis related thrombotic total occlusion of MPV and treated with TIPS from January 2000 to January 2010 were retrospectively analyzed. Twenty-three (23.5%) patients had MPV (single site) thrombosis, 55 (56.1%) had multiple site-thrombosis (MPV and other), 17 (17.3%) had cavernous transformation of portal vein, and 3 (3.1%) had post-transplant thrombosis. The successful rate of TIPS was 90.7%, without any procedure-related deaths or severe complications. Mean portal pressure was dropped from 33.08 ± 1.38 mmHg preoperatively to 20.18 ± 0.83 mmHg postoperatively (p < 0.001). Collectively, TIPS is safe and effective in treating liver cirrhosis-related thrombotic total occlusion of MPV. This complex procedure requires combination of indirect portography and percutaneous transhepatic portal techniques to increase the rate of success.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
