

The Pattern of Retinal Nerve Fiber Layer and Macular Ganglion Cell-Inner Plexiform Layer Thickness Changes in Glaucoma
- PMID: 28884025
- PMCID: PMC5572589
- DOI: 10.1155/2017/6078365
The Pattern of Retinal Nerve Fiber Layer and Macular Ganglion Cell-Inner Plexiform Layer Thickness Changes in Glaucoma
Abstract
Background/aims: To investigate the patterns of retinal ganglion cell damage at different stages of glaucoma, using the circumpapillary retinal nerve fiber layer (RNFL) and macula ganglion cell-inner plexiform layer (GCIPL) thicknesses.
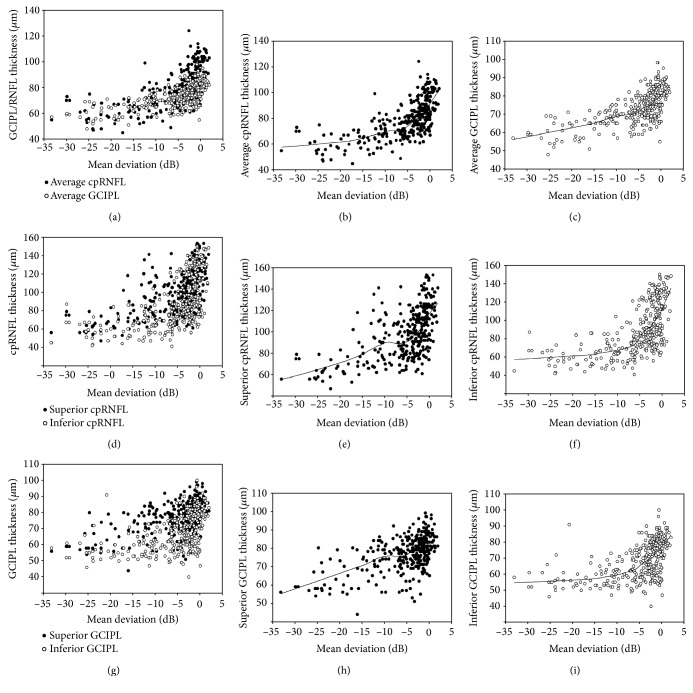
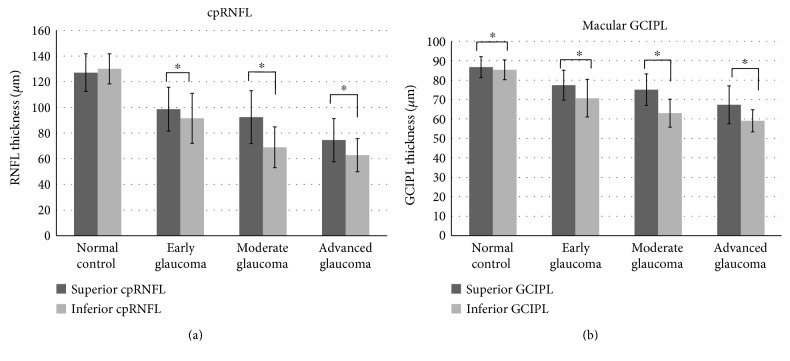
Methods: In 296 eyes of 296 glaucoma patients and 55 eyes of 55 healthy controls, the correlations of mean deviation (MD) with the superior and inferior quadrant RNFL/GCIPL thickness (defined as the average of three superior and inferior sectors, resp.) were analyzed.
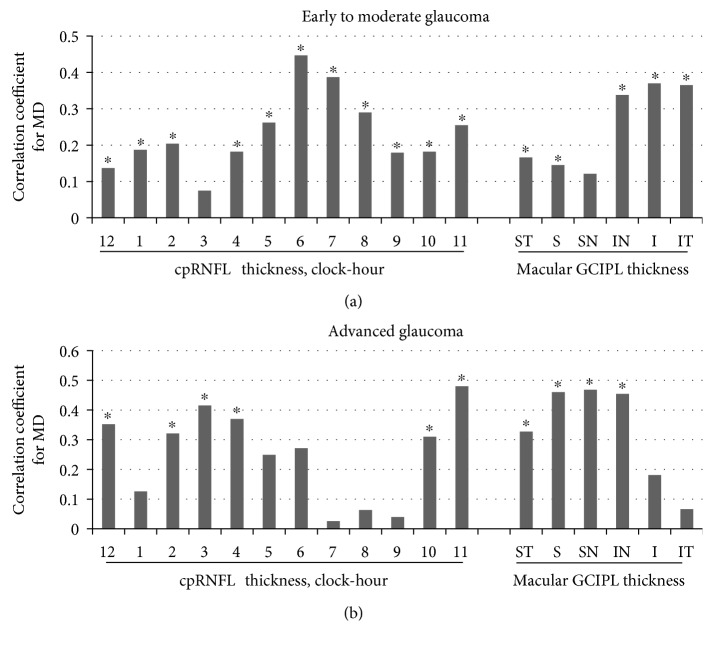
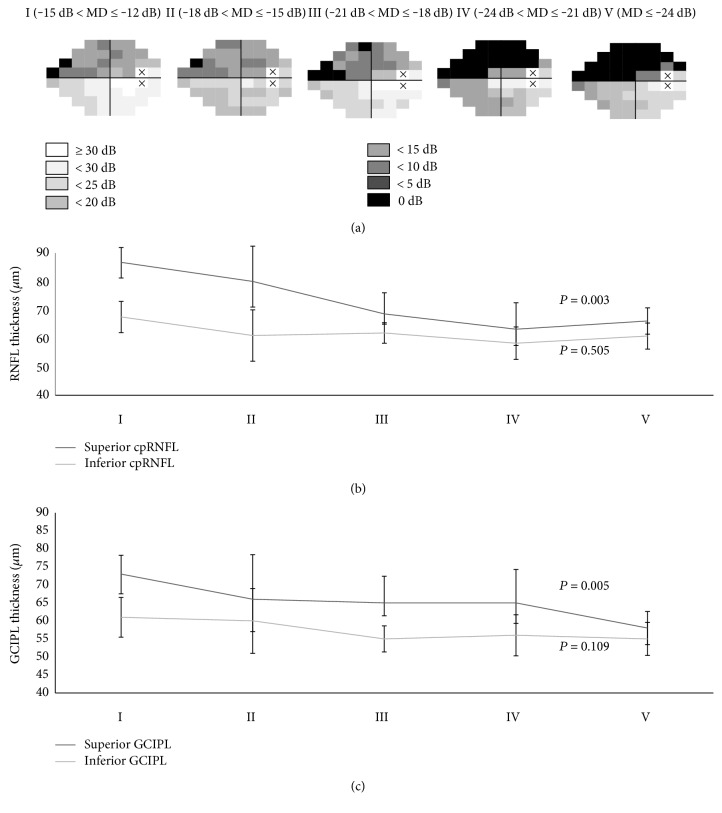
Results: In early to moderate glaucoma, most of the RNFL/GCIPL thicknesses had significant positive correlations with the MD. In advanced glaucoma, the superior GCIPL thickness showed the highest correlation with MD (r = 0.495), followed by the superior RNFL (r = 0.452) (all; P < 0.05). The correlation coefficient of the inferior RNFL thickness with MD (r < 0.471) was significantly stronger in early to moderate glaucoma compared to that in advanced glaucoma (r = 0.192; P < 0.001). In contrast, the correlations of the superior GCIPL thickness with MD (r = 0.452) in advanced glaucoma was significantly stronger compared to that in early to moderate glaucoma (r = 0.159; P < 0.001).
Conclusions: The most preserved region in advanced glaucoma appears to be the superior macular GCIPL, whereas the most vulnerable region for initial glaucoma is the inferior RNFL around the optic disc.
Figures
Similar articles
-
Comparing the Rates of Retinal Nerve Fiber Layer and Ganglion Cell-Inner Plexiform Layer Loss in Healthy Eyes and in Glaucoma Eyes.Am J Ophthalmol. 2017 Jun;178:38-50. doi: 10.1016/j.ajo.2017.03.008. Epub 2017 Mar 16. Am J Ophthalmol. 2017. PMID: 28315655
-
Structural measurements and vessel density of spectral-domain optic coherence tomography in early, moderate, and severe primary angle-closure glaucoma.Int J Ophthalmol. 2023 Jul 18;16(7):1100-1109. doi: 10.18240/ijo.2023.07.15. eCollection 2023. Int J Ophthalmol. 2023. PMID: 37465514 Free PMC article.
-
Ganglion cell-inner plexiform layer and retinal nerve fiber layer thickness according to myopia and optic disc area: a quantitative and three-dimensional analysis.BMC Ophthalmol. 2017 Mar 11;17(1):22. doi: 10.1186/s12886-017-0419-1. BMC Ophthalmol. 2017. PMID: 28283025 Free PMC article.
-
Patterns of glaucoma progression in retinal nerve fiber and macular ganglion cell-inner plexiform layer in spectral-domain optical coherence tomography.Jpn J Ophthalmol. 2017 Jul;61(4):324-333. doi: 10.1007/s10384-017-0511-3. Epub 2017 Apr 3. Jpn J Ophthalmol. 2017. PMID: 28374270
-
Ganglion Cell Complex Analysis: Correlations with Retinal Nerve Fiber Layer on Optical Coherence Tomography.Diagnostics (Basel). 2023 Jan 11;13(2):266. doi: 10.3390/diagnostics13020266. Diagnostics (Basel). 2023. PMID: 36673076 Free PMC article. Review.
Cited by
-
The "Topography" of Glaucomatous Defect Using OCT and Visual Field Examination.J Curr Glaucoma Pract. 2022 Jan-Apr;16(1):31-35. doi: 10.5005/jp-journals-10078-1353. J Curr Glaucoma Pract. 2022. PMID: 36060037 Free PMC article.
-
One-Year Outcomes of Second-Generation Trabecular Micro-Bypass Stents (iStent Inject) Implantation with Cataract Surgery in Different Glaucoma Subtypes and Severities.Ophthalmol Ther. 2019 Dec;8(4):563-575. doi: 10.1007/s40123-019-00214-z. Epub 2019 Sep 19. Ophthalmol Ther. 2019. PMID: 31538316 Free PMC article.
-
Optic nerve head vessel density in different stages of pseudoexfoliation disease.Br J Ophthalmol. 2022 Feb;106(2):223-228. doi: 10.1136/bjophthalmol-2020-317605. Epub 2020 Nov 27. Br J Ophthalmol. 2022. PMID: 33246938 Free PMC article.
-
Percentage macular ganglion cell complex and peripapillary retinal nerve fiber layer loss in different stages of glaucoma.Indian J Ophthalmol. 2025 Mar 1;73(Suppl 2):S308-S312. doi: 10.4103/IJO.IJO_3238_23. Epub 2025 Feb 21. Indian J Ophthalmol. 2025. PMID: 39982090 Free PMC article.
-
Focal alteration of the intraretinal layers in neurodegenerative disorders.Ann Eye Sci. 2020 Mar;5:8. doi: 10.21037/aes.2019.12.04. Ann Eye Sci. 2020. PMID: 32939442 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
