

New Insights about Pulmonary Epithelioid Hemangioendothelioma: Review of the Literature and Two Case Reports
- PMID: 28884037
- PMCID: PMC5573100
- DOI: 10.1155/2017/5972940
New Insights about Pulmonary Epithelioid Hemangioendothelioma: Review of the Literature and Two Case Reports
Abstract
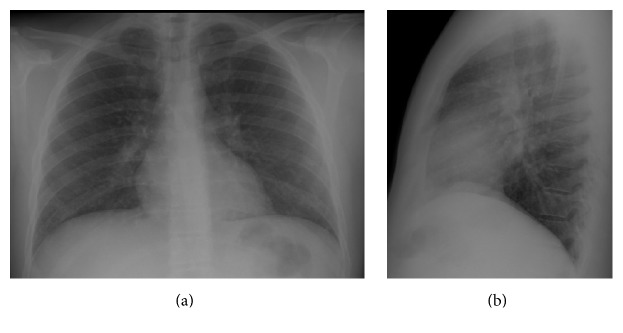
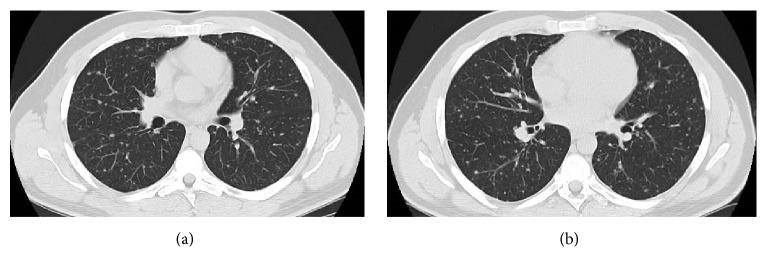
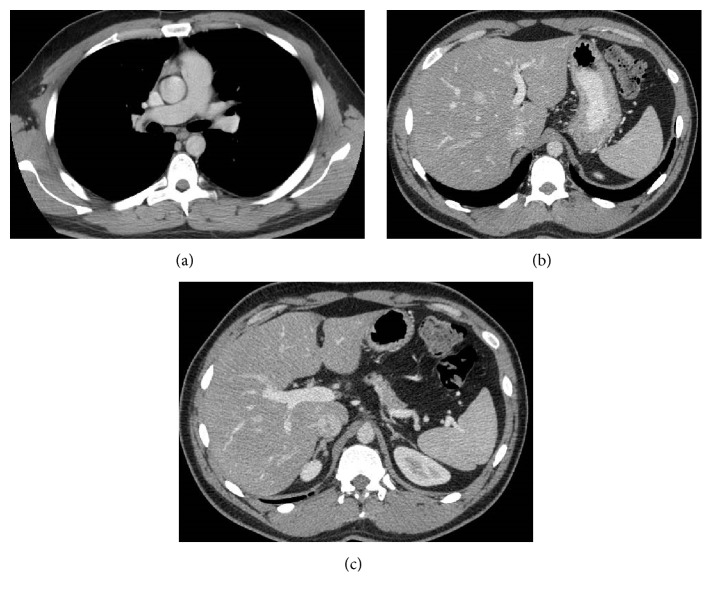
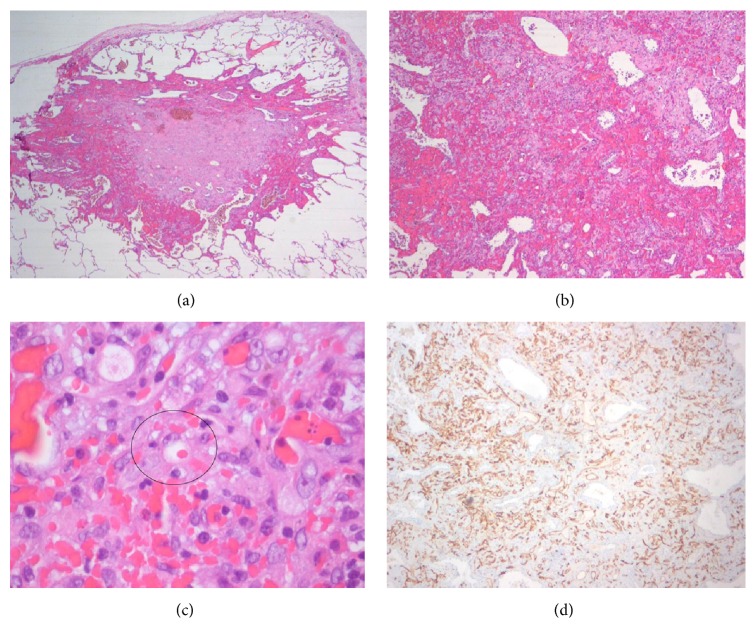
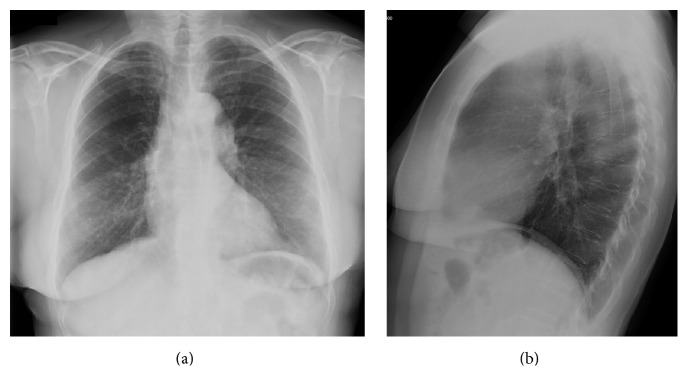
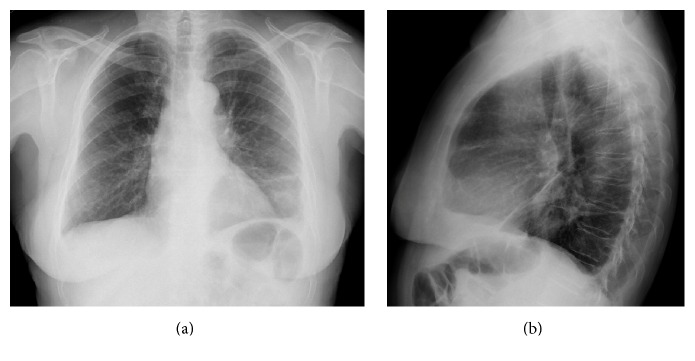
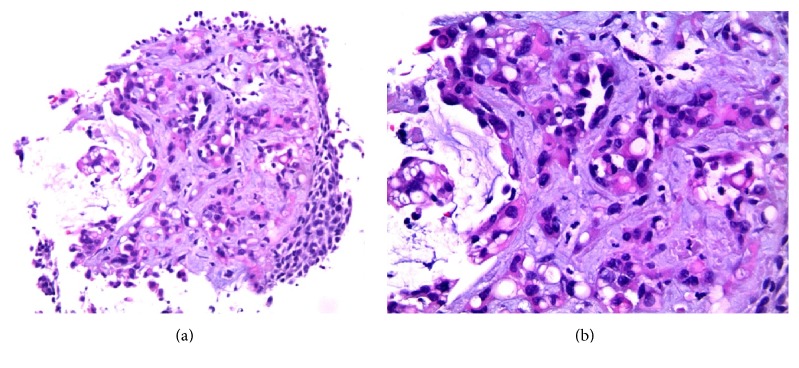
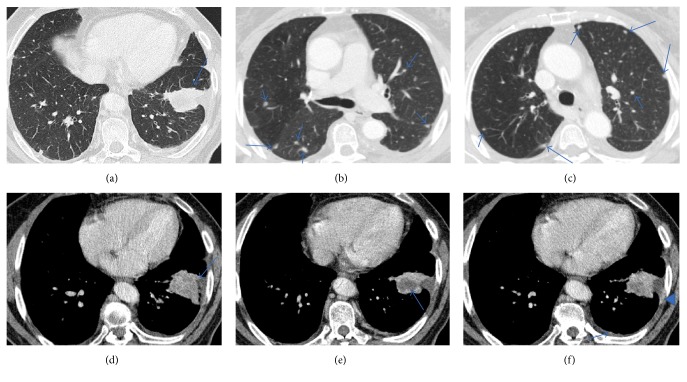
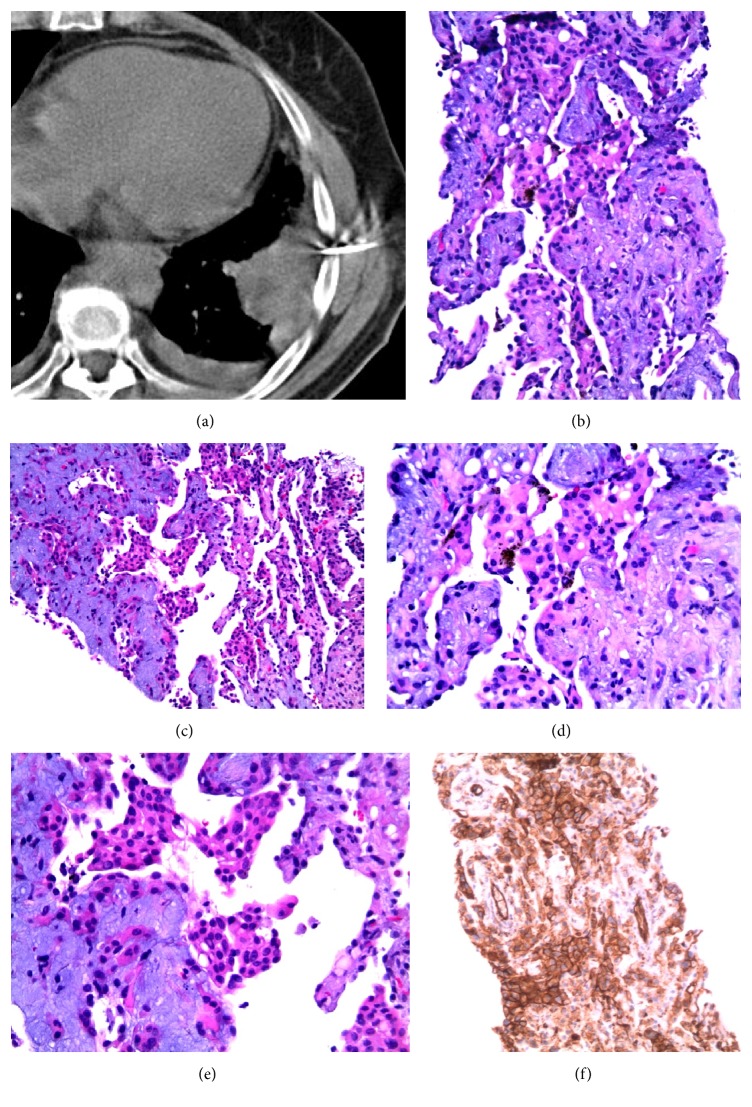
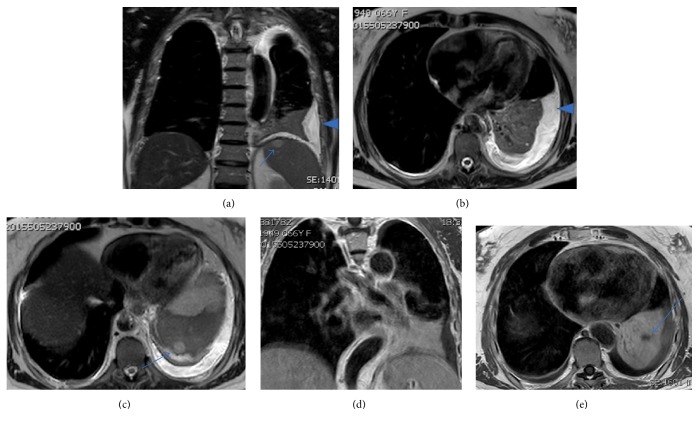
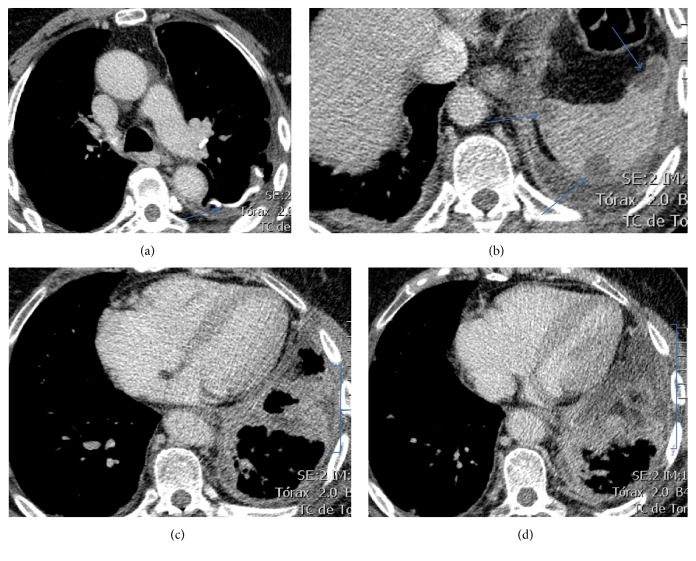
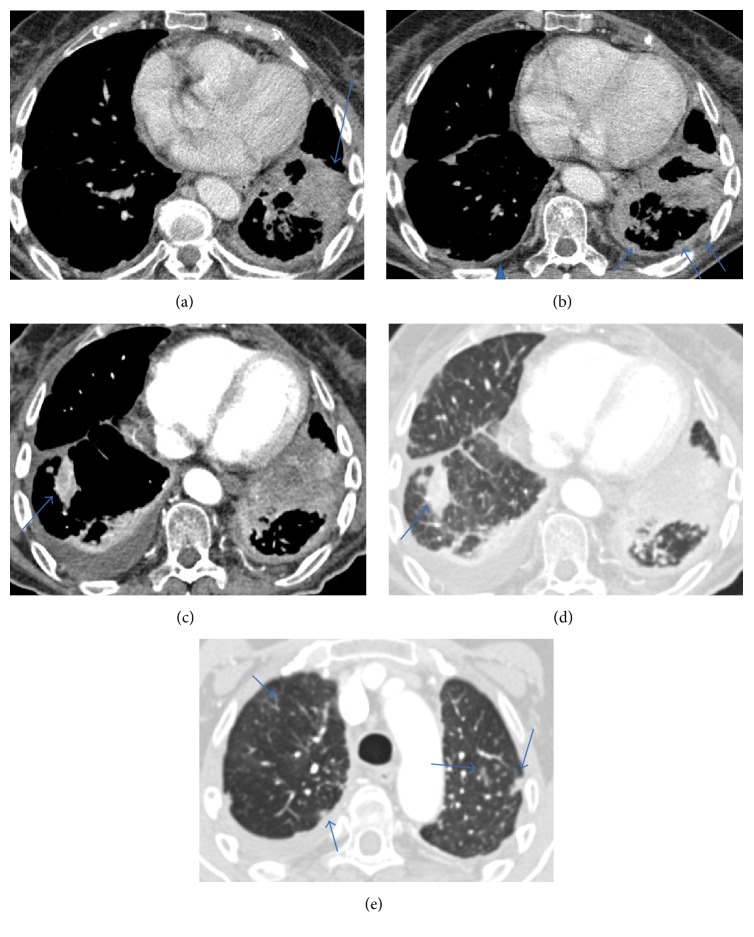
Pulmonary epithelioid hemangioendothelioma (PEH) is a rare neoplasm of vascular origin. There are three different major imaging patterns identified in thoracic manifestation of epithelioid hemangioendothelioma: (1) multiple pulmonary nodules; (2) multiple pulmonary reticulonodular opacities; and (3) diffuse infiltrative pleural thickening. Radiographically, presence of bilateral multiple nodules is the most common pattern of presentation. The diagnosis is made on the basis of histopathological findings and confirmed by positive immunohistochemistry staining. Although the prognostic factors for PEH have not yet been well established, a better prognosis is usually associated with the multinodular pattern. We report two different imagological presentations of this rare disease, based on two institutional experiences, along with a review of the relevant literature.
Figures
References
-
- Weiss S. W., Ishak K. G., Dail D. H., Sweet D. E., Enzinger F. M. Epithelioid hemangioendothelioma and related lesions. Semin Diagn Pathol. 1986;3(4):259–287. http://www.ncbi.nlm.nih.gov/pubmed/3303234. - PubMed
-
- Dail D. H., Liebow A. A., Gmelich J. T., et al. Intravascular, bronchiolar, and alveolar tumor of the lung (IVBAT): An analysis of twenty cases of a peculiar sclerosing endothelial tumor. Cancer. 1983;51(3):452–464. doi: 10.1002/1097-0142(19830201)51:3<452::AID-CNCR2820510317>3.0.CO;2-M. doi: 10.1002/1097-0142(19830201)51:3<452::AID-CNCR2820510317>3.0.CO;2-M. - DOI - PubMed
-
- de Albuquerque A. K. A. C., Romano S. d. O., Eisenberg A. L. A. Epithelioid hemangioendothelioma: 15 years at the National Cancer Institute. Literature review. Brazilian Journal of Pathology and Laboratory Medicine. 2013;49(2):119–125. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1676-2444201....
-
- Fletcher C. D. M., Bridge J. A., Hogendoorn PCW M. F. WHO Classification of Tumours of Soft Tissue and Bone. 4th. Vol. 5. WHO/IARC Classification of Tumours; 2013. http://publications.iarc.fr/Book-And-Report-Series/Who-Iarc-Classificati....
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
