

Time-to-event analysis of surgically treated posthemorrhagic hydrocephalus in preterm infants: a single-institution retrospective study
- PMID: 28884229
- PMCID: PMC5647248
- DOI: 10.1007/s00381-017-3588-6
Time-to-event analysis of surgically treated posthemorrhagic hydrocephalus in preterm infants: a single-institution retrospective study
Abstract
Purpose: The purpose of this study is to report time points relevant to the neurosurgical management of posthemorrhagic hydrocephalus (PHH).
Methods: Data were collected retrospectively on 104 preterm infants with intraventricular hemorrhage (IVH) who received neurosurgical intervention for PHH at St. Louis Children's Hospital from 1994 to 2016. Kaplan-Meier curves were constructed for various endpoints.
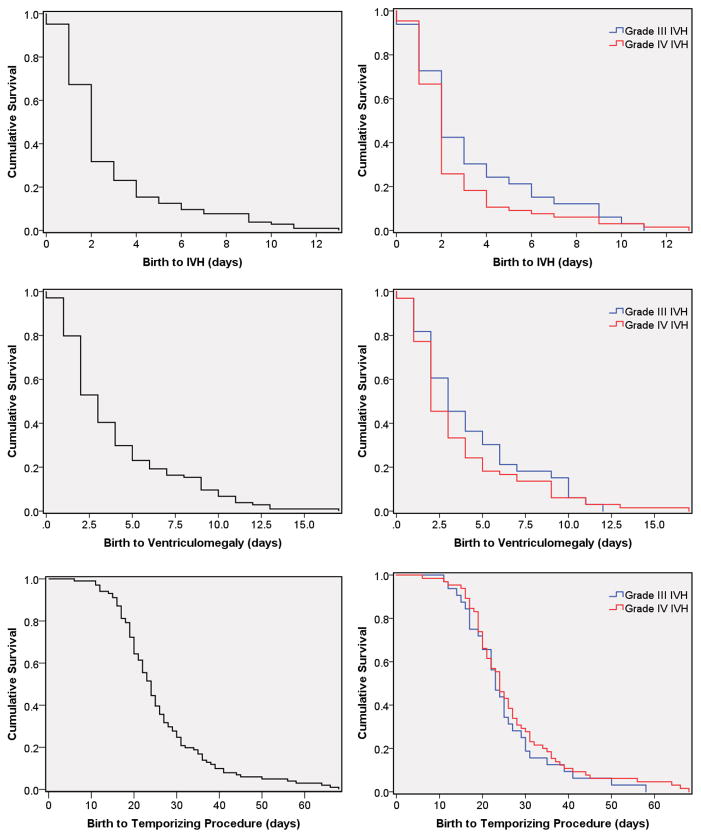
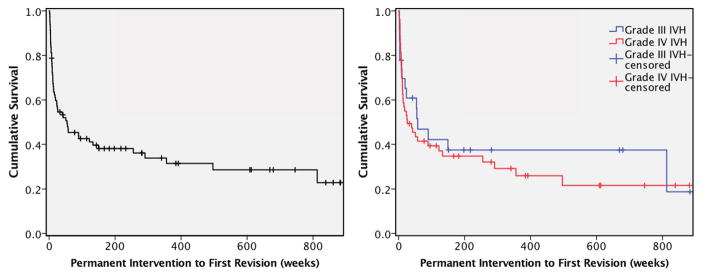
Results: IVH grade on head ultrasound obtained through routine clinical care was II, III, and IV in 5 (4.8%), 33 (31.7%), and 66 (63.5%) of the patients, respectively. Neither IVH size nor location appeared to affect development of PHH. Days from birth to IVH, ventriculomegaly, temporizing neurosurgical procedure (TNP), and permanent neurosurgical intervention were 2.0 (95% CI 1.7-2.3), 3.0 (2.5-3.5), 24.0 (22.2-25.8), and 101.0 (90.4-111.6), respectively. Grades III and IV IVH did not differ in age at IVH diagnosis (Χ 2 (1 d.f.) = 1.32, p = 0.25), ventriculomegaly (Χ 2 = 0.73, p = 0.40), TNP (Χ 2 = 0.61, p = 0.43), or permanent intervention (Χ 2 = 2.48, p = 0.17). Ventricular reservoirs and ventriculosubgaleal shunts were used in 71 (68.3%) and 30 (28.8%), respectively. Eighty (76.9%) of the patients ultimately received a VPS. Five (4.8%) underwent a primary endoscopic third ventriculostomy (ETV), and two (1.9%) had ETV for a revision procedure. Four of the seven ETVs had choroid plexus cauterization.
Conclusions: Although most infants who develop IVH and ventriculomegaly will do so within a few days of birth, at-risk infants should be observed for at least 4 weeks with serial head ultrasounds to monitor for PHH requiring surgery.
Keywords: Intraventricular hemorrhage; Temporizing neurosurgical procedure; Ventriculomegaly; Ventriculoperitoneal shunt.
Figures



References
-
- Beverley DW, Chance GW, Coates CF. Intraventricular haemorrhage--timing of occurrence and relationship to perinatal events. Br J Obstet Gynaecol. 1984;91:1007–1013. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
