

Pulmonary large cell neuroendocrine carcinoma with adenocarcinoma-like features: napsin A expression and genomic alterations
- PMID: 28884744
- PMCID: PMC5937126
- DOI: 10.1038/modpathol.2017.110
Pulmonary large cell neuroendocrine carcinoma with adenocarcinoma-like features: napsin A expression and genomic alterations
Abstract
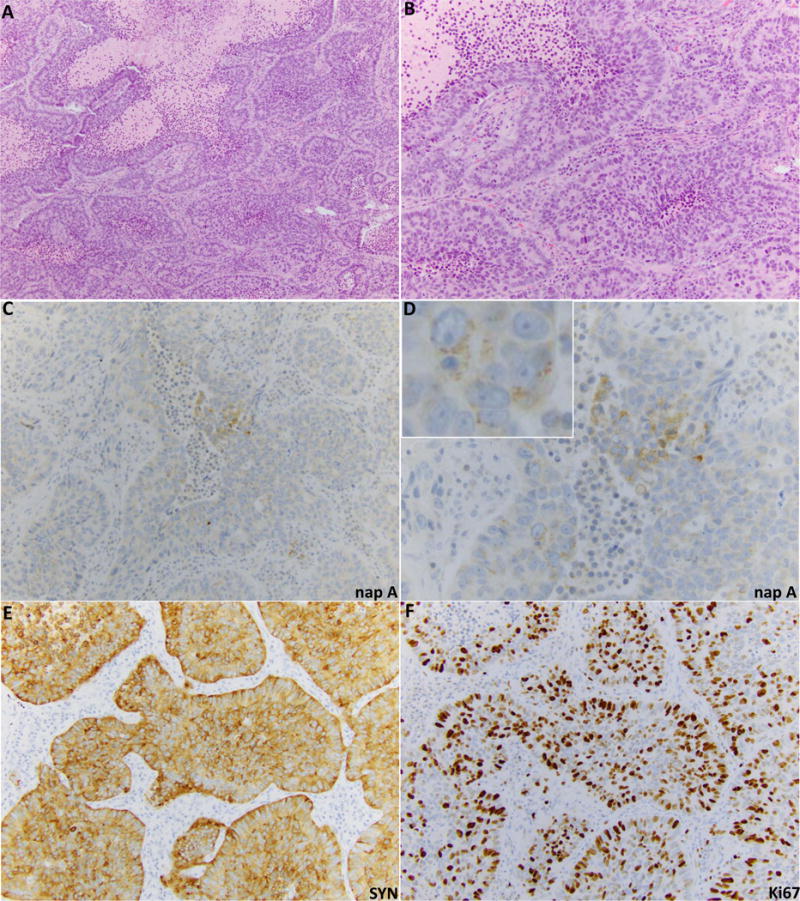
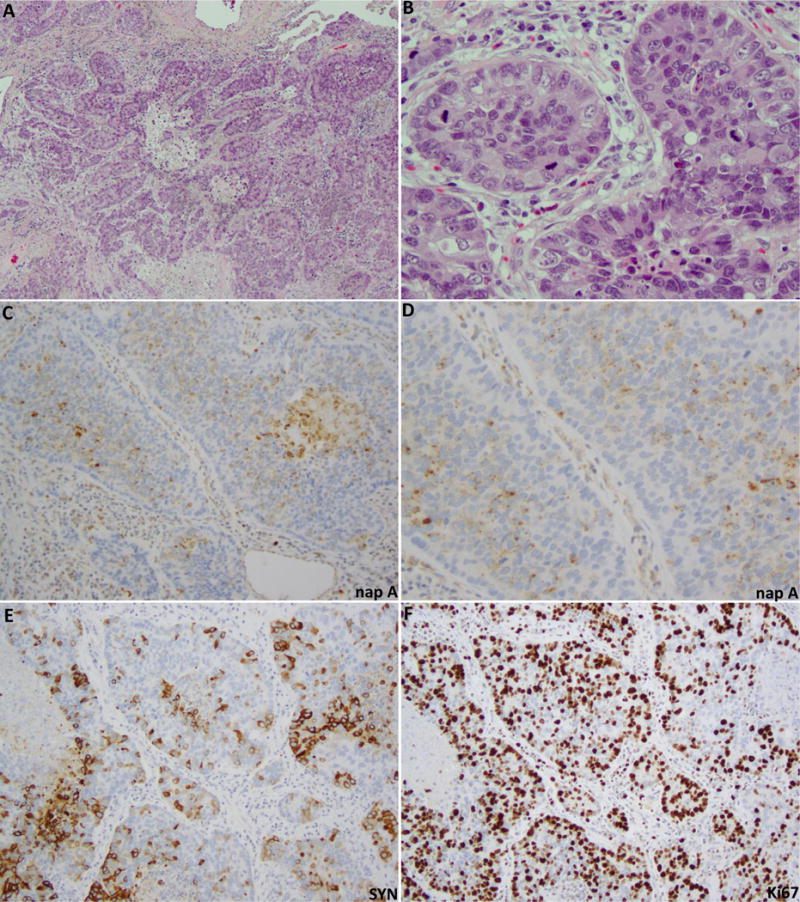
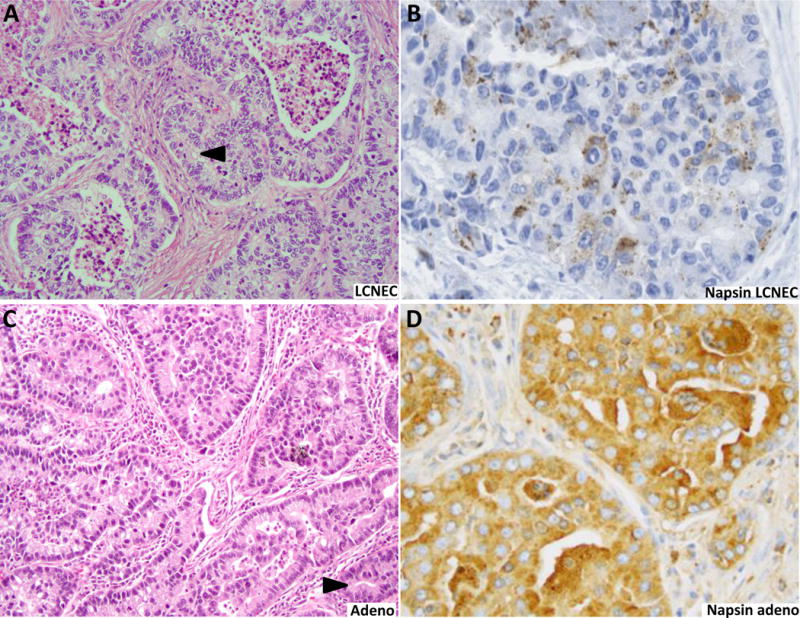
Pulmonary large cell neuroendocrine carcinoma (LCNEC) is a highly aggressive malignancy, which was recently found to comprise three major genomic subsets: small cell carcinoma-like, non-small cell carcinoma (predominantly adenocarcinoma)-like, and carcinoid-like. To further characterize adenocarcinoma-like subset, here we analyzed the expression of exocrine marker napsin A, along with TTF-1, in a large series of LCNECs (n=112), and performed detailed clinicopathologic and genomic analysis of napsin A-positive cases. For comparison, we analyzed napsin A expression in other lung neuroendocrine neoplasms (177 carcinoids, 37 small cell carcinomas) and 60 lung adenocarcinomas. We found that napsin A was expressed in 15% of LCNEC (17/112), whereas all carcinoids and small cell carcinomas were consistently negative. Napsin A reactivity in LCNEC was focal in 12/17 cases, and weak or moderate in intensity in all cases, which was significantly lower in the extent and intensity than seen in adenocarcinomas (P<0.0001). The combination of TTF-1-diffuse/napsin A-negative or focal was typical of LCNEC but was rare in adenocarcinoma, and could thus serve as a helpful diagnostic clue. The diagnosis of napsin A-positive LCNECs was confirmed by classic morphology, diffuse labeling for at least one neuroendocrine marker, most consistently synaptophysin, and the lack of distinct adenocarcinoma component. Genomic analysis of 14 napsin A-positive LCNECs revealed the presence of mutations typical of lung adenocarcinoma (KRAS and/or STK11) in 11 cases. In conclusion, LCNECs are unique among lung neuroendocrine neoplasms in that some of these tumors exhibit low-level expression of exocrine marker napsin A, and harbor genomic alterations typical of adenocarcinoma. Despite the apparent close biological relationship, designation of adeno-like LCNEC as a separate entity from adenocarcinoma is supported by their distinctive morphology, typically diffuse expression of neuroendocrine marker(s) and aggressive behavior. Further studies are warranted to assess the clinical utility and optimal method of identifying adenocarcinoma-like and other subsets of LCNEC in routine practice.
Conflict of interest statement
Figures
References
-
- Rekhtman N. Neuroendocrine tumors of the lung: an update. Arch Pathol Lab Med. 2010;134:1628–1638. - PubMed
-
- Brambilla E, Beasley MB, Chirieac LR, et al. Large cell neuroendocrine carcinoma. In: Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG, editors. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. Lyon: IARC Press; 2015. pp. 69–72.
-
- den Bakker MA, Willemsen S, Grunberg K, et al. Small cell carcinoma of the lung and large cell neuroendocrine carcinoma interobserver variability. Histopathology. 2010;56:356–363. - PubMed
-
- Jiang SX, Kameya T, Shoji M, Dobashi Y, Shinada J, Yoshimura H. Large cell neuroendocrine carcinoma of the lung: a histologic and immunohistochemical study of 22 cases. Am J Surg Pathol. 1998;22:526–537. - PubMed
-
- Travis WD, Gal AA, Colby TV, Klimstra DS, Falk R, Koss MN. Reproducibility of neuroendocrine lung tumor classification. Hum Pathol. 1998;29:272–279. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
