

Evidence for Persistent Immune Suppression in Patients Who Develop Chronic Critical Illness After Sepsis
- PMID: 28885387
- PMCID: PMC5809297
- DOI: 10.1097/SHK.0000000000000981
Evidence for Persistent Immune Suppression in Patients Who Develop Chronic Critical Illness After Sepsis
Abstract
Background: Many sepsis survivors develop chronic critical illness (CCI) and are assumed to be immunosuppressed, but there is limited clinical evidence to support this. We sought to determine whether the incidence of secondary infections and immunosuppressive biomarker profiles of patients with CCI differ from those with rapid recovery (RAP) after sepsis.
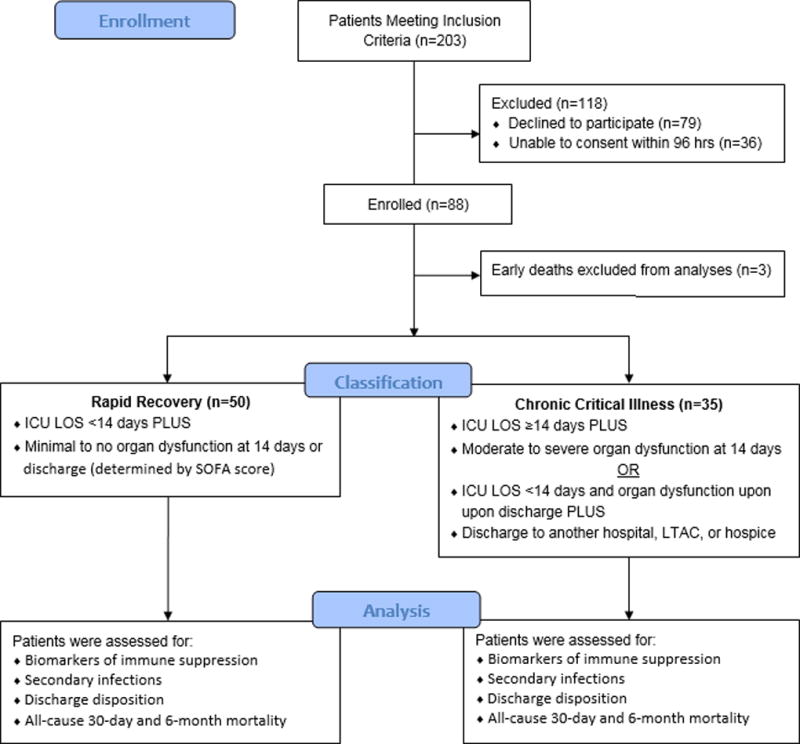
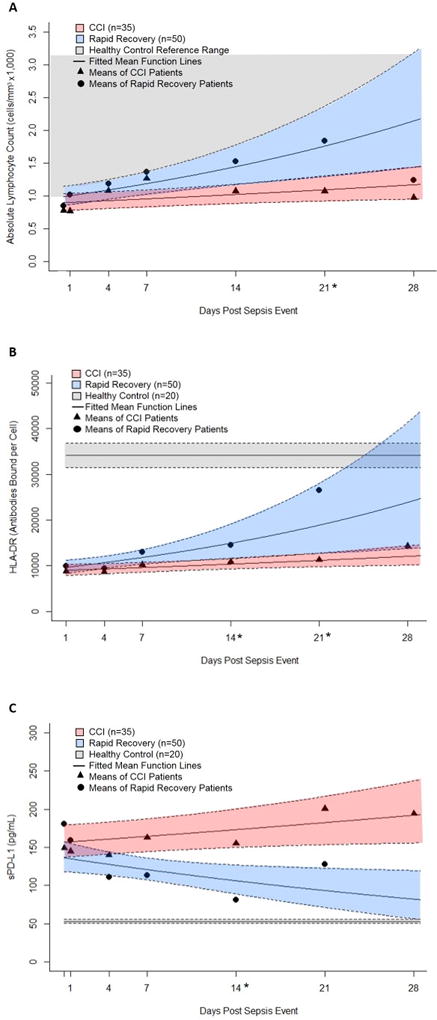
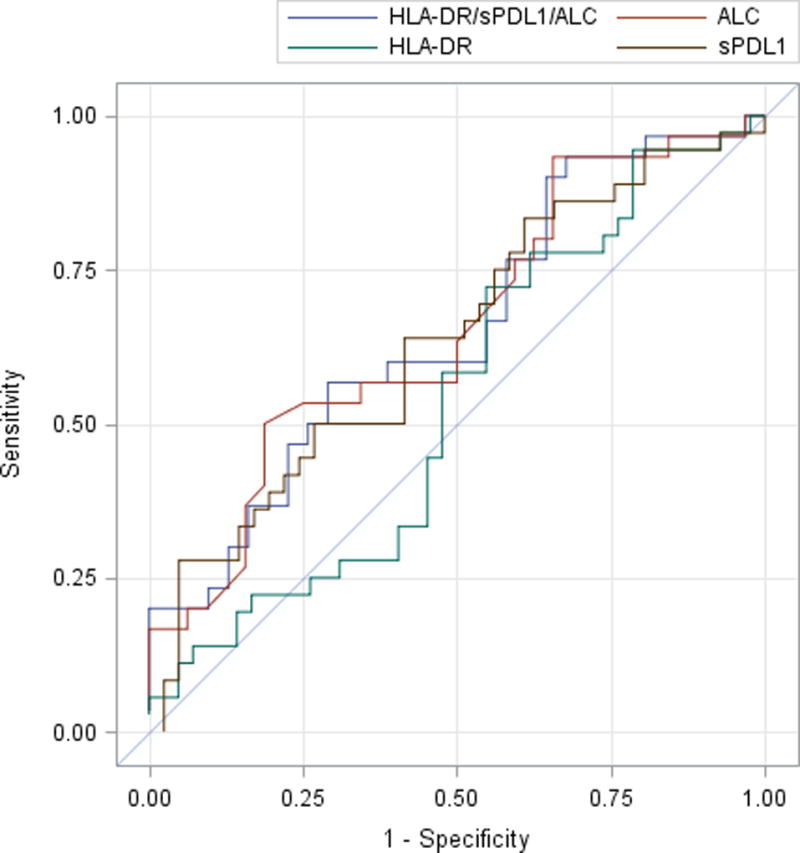
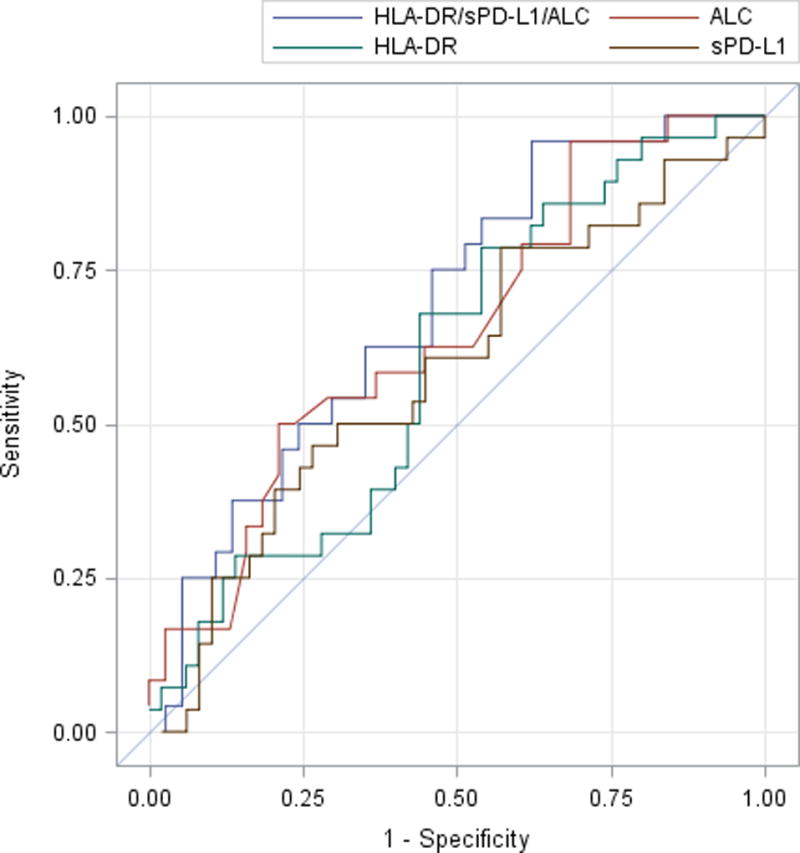
Methods: This prospective observational study evaluated 88 critically ill patients with sepsis and 20 healthy controls. Cohorts were defined based on clinical trajectory (early death, RAP, or CCI), whereas immunosuppression was clinically determined by the presence of a postsepsis secondary infection. Serial blood samples were collected for absolute lymphocyte counts (ALCs), monocytic human leukocyte antigen-DR (mHLA-DR) expression, and plasma-soluble programmed death-ligand 1 (sPD-L1) concentrations.
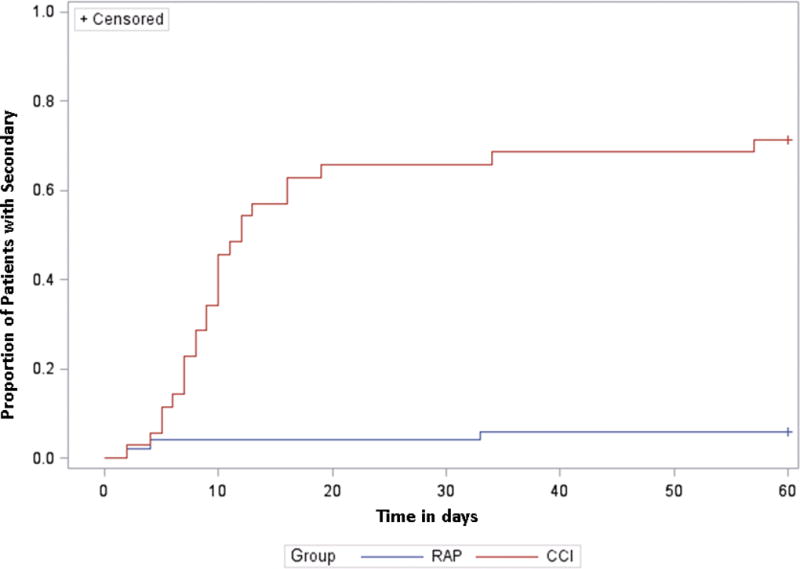
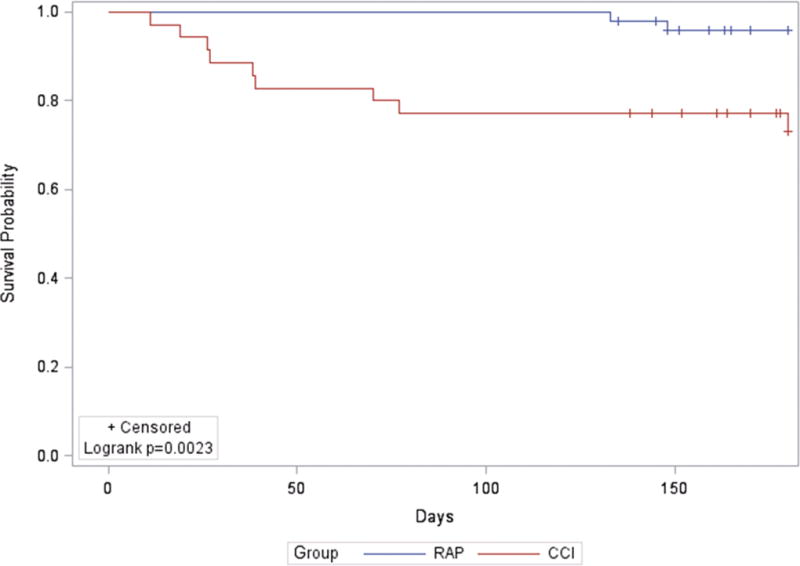
Results: Of the 88 patients with sepsis, 3 (3%) died within 14 days of sepsis onset, 50 (57%) experienced RAP, and 35 (40%) developed CCI. Compared with RAP patients, CCI patients exhibited a higher incidence and overall number of infections adjusted for hospital length of stay. ALC and mHLA-DR levels were dramatically reduced at the time of sepsis diagnosis when compared with healthy controls, whereas sPD-L1 concentrations were significantly elevated. There were no differences between RAP and CCI patients in ALC, sPD-L1, or mHLA-DR at the time of diagnosis or within 24 h after sepsis diagnosis. However, in contrast to the RAP group, CCI patients failed to exhibit any trend toward restoration of normal values of ALC, HLA-DR, and sPD-L1.
Conclusions: Septic patients demonstrate clinical and biological evidence to suggest they are immunosuppressed at the time of sepsis diagnosis. Those who develop CCI have a greater incidence of secondary infections and persistently aberrant markers of impaired host immunity, although measurements at the time of sepsis onset did not distinguish between subjects with RAP and CCI.
Figures
References
-
- Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA. 2014;311(13):1308–1316. - PubMed
-
- Budde K, Matz M, Durr M, Glander P. Biomarkers of over-immunosuppression. Clin Pharmacol Ther. 2011;90(2):316–322. - PubMed
-
- Fraser DR, Dombrovskiy VY, Vogel TR. Infectious complications after vehicular trauma in the United States. Surg Infect (Larchmt) 2011;12(4):291–296. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
