

Complement (C1q) Binding De Novo Donor-Specific Antibodies and Cardiac-Allograft Vasculopathy in Pediatric Heart Transplant Recipients
- PMID: 28885488
- PMCID: PMC5820172
- DOI: 10.1097/TP.0000000000001944
Complement (C1q) Binding De Novo Donor-Specific Antibodies and Cardiac-Allograft Vasculopathy in Pediatric Heart Transplant Recipients
Abstract
Background: We hypothesized C1q binding de novo donor-specific antibody (DSA) after heart transplant (HT) is a higher risk for development of coronary artery vasculopathy (CAV) in children.
Methods: A retrospective analysis of 127 pediatric HT recipients transplanted between January 2005 and December 2014 was used to determine complement (C1q)-binding de novo DSA on the outcomes of HT and the ability of the C1q assay to predict CAV development.
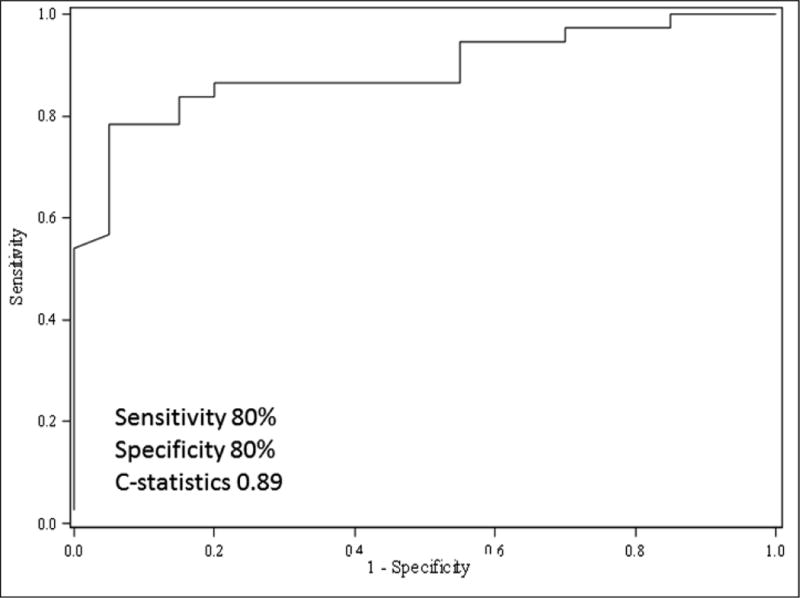
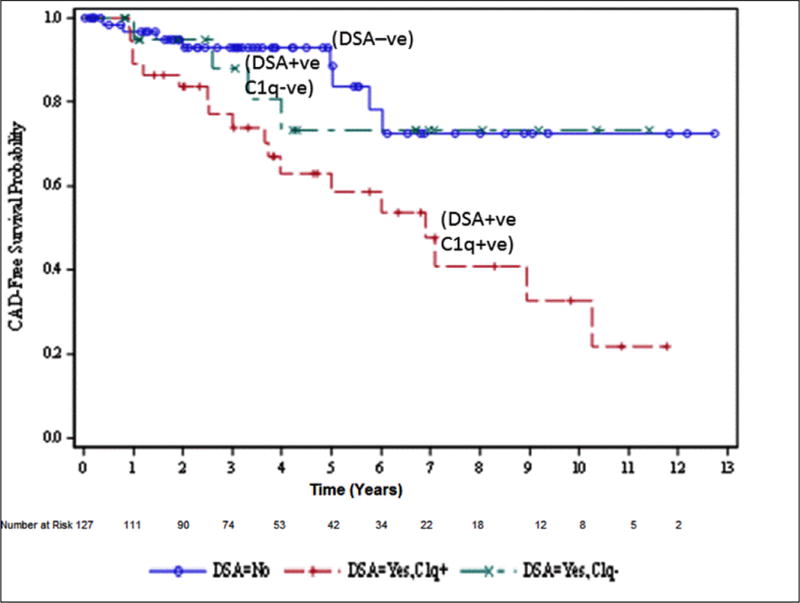
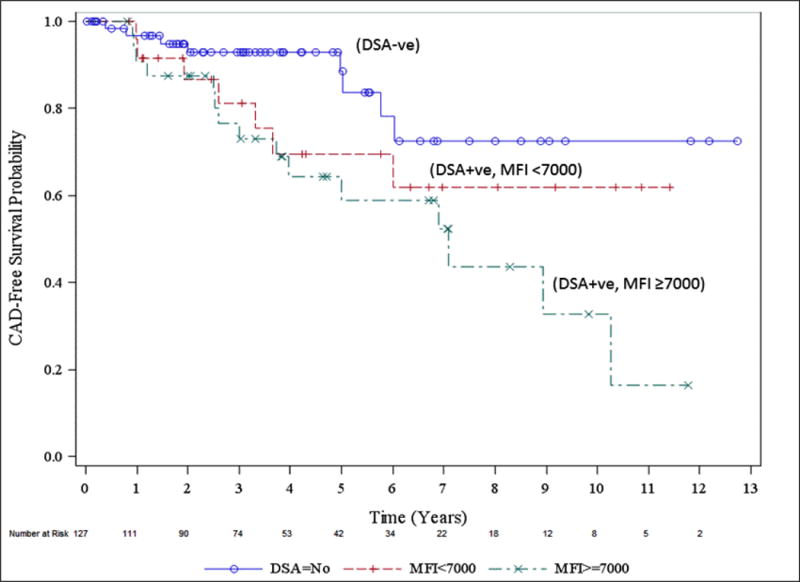
Results: Of 127 patients, 59 (46.4%) developed de novo DSA, 37 of those had C1q+ DSA. There was no difference in baseline characteristics except patients who developed C1q+ DSA more often received a donor heart from a female compared with C1q- DSA group (P = 0.034). The DSA median fluorescent intensity (MFI) value of 7000 or greater had 80% sensitivity and 80% specificity (C statistics 0.89, P <0.05) for predicting positive C1q binding. Multivariate analyses identified C1q binding DSA as an independent risk for CAV with a hazard ratio (HR) of 3.25 (95% confidence interval [CI], 1.33-7.93; P = 0.0095). In multivariable Cox proportional hazard models, the covariates associated with graft loss included: C1q+ DSA (HR, 3.2; 95% CI, 1.34-7.86; P < 0.009), pre-HT renal insufficiency (HR, 11.3; 95% CI, 3.71-34.29; P < 0.0001), and pre-HT ventilator support (HR, 3.3; 95% CI, 1.39-7.81; P = 0.007).
Conclusions: The DSA strength in MFI correlates with positive C1q-binding activity and hence functional capabilities of DSA. Close monitoring of DSA strength in MFI and function (C1q assay) may be useful for identifying pediatric HT recipient at risk for development of CAV.
Conflict of interest statement
The authors declare no conflicts of interest
Figures
Similar articles
-
The role of immunoglobulin-G subclasses and C1q in de novo HLA-DQ donor-specific antibody kidney transplantation outcomes.Transplantation. 2013 May 15;95(9):1113-9. doi: 10.1097/TP.0b013e3182888db6. Transplantation. 2013. PMID: 23514959
-
The role of complement-fixing donor-specific antibodies identified by a C1q assay after heart transplantation.Clin Transplant. 2017 Nov;31(11). doi: 10.1111/ctr.13121. Epub 2017 Oct 15. Clin Transplant. 2017. PMID: 28940521 Clinical Trial.
-
Donor-specific HLA alloantibodies: Impact on cardiac allograft vasculopathy, rejection, and survival after pediatric heart transplantation.J Heart Lung Transplant. 2016 Jan;35(1):87-91. doi: 10.1016/j.healun.2015.08.008. Epub 2015 Sep 3. J Heart Lung Transplant. 2016. PMID: 26422083
-
Relationship among C1q-fixing de novo donor specific antibodies, C4d deposition and renal outcome in transplant glomerulopathy.Transpl Immunol. 2015 Sep;33(1):7-12. doi: 10.1016/j.trim.2015.06.002. Epub 2015 Jul 6. Transpl Immunol. 2015. PMID: 26160049 Review.
-
Application, technical issues, and interpretation of C1q for graft outcome.Curr Opin Organ Transplant. 2017 Oct;22(5):505-510. doi: 10.1097/MOT.0000000000000454. Curr Opin Organ Transplant. 2017. PMID: 28723698 Free PMC article. Review.
Cited by
-
Molecular Signature of Antibody-Mediated Chronic Vasculopathy in Heart Allografts in a Novel Mouse Model.Am J Pathol. 2022 Jul;192(7):1053-1065. doi: 10.1016/j.ajpath.2022.04.003. Epub 2022 Apr 29. Am J Pathol. 2022. PMID: 35490714 Free PMC article.
-
Carbohydrate Metabolism Disorders in Relation to Cardiac Allograft Vasculopathy (CAV) Intensification in Heart Transplant Patients According to the Grading Scheme Developed by the International Society for Heart and Lung Transplantation (ISHLT).Ann Transplant. 2022 Feb 15;27:e933420. doi: 10.12659/AOT.933420. Ann Transplant. 2022. PMID: 35165250 Free PMC article.
-
Non-invasive cardiac allograft rejection surveillance: reliability and clinical value for prevention of heart failure.Heart Fail Rev. 2021 Mar;26(2):319-336. doi: 10.1007/s10741-020-10023-3. Epub 2020 Sep 5. Heart Fail Rev. 2021. PMID: 32889634 Review.
-
Bringing Clarity to the Murky Problem of Cardiac Allograft Vasculopathy.Am J Pathol. 2022 Jul;192(7):986-989. doi: 10.1016/j.ajpath.2022.05.002. Epub 2022 May 14. Am J Pathol. 2022. PMID: 35577009 Free PMC article. No abstract available.
-
De Novo Complement-Binding Anti-HLA Antibodies in Heart Transplanted Patients Is Associated with Severe Cardiac Allograft Vasculopathy and Poor Long-Term Survival.J Clin Med. 2022 Jun 28;11(13):3731. doi: 10.3390/jcm11133731. J Clin Med. 2022. PMID: 35807015 Free PMC article.
References
-
- Ho EK, Vlad G, Vasilescu ER, et al. Pre- and post-transplantation allosensitization in heart allograft recipients: major impact of de novo alloantibody production on allograft survival. Hum Immunol. 2011;72(1):5–10. - PubMed
-
- Tran A, Fixler D, Huang R, Meza T, Lacelle C, Das B. Donor-specific HLA alloantibodies: Impact on cardiac allograft vasculopathy, rejection, and survival after pediatric heart transplantation. J Heart Lung Transplant. 2016;35(1):87–91. - PubMed
-
- Chin C, Chen G, Sequeria F, et al. Clinical usefulness of a novel C1q assay to detect immunoglobulin G antibodies capable of fixing complement in sensitized pediatric heart transplant patients. J Heart Lung Transplant. 2011;30(2):158–63. - PubMed
-
- Sutherland SM, Chen G, Sequeira FA, Lou CD, Alexander SR, Tyan DB. Complement-fixing donor-specific antibodies identified by a novel C1q assay are associated with allograft loss. Pediatric Transplant. 2012;16(1):12–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
