

An Australian general practice based strategy to improve chronic disease prevention, and its impact on patient reported outcomes: evaluation of the preventive evidence into practice cluster randomised controlled trial
- PMID: 28886739
- PMCID: PMC5591527
- DOI: 10.1186/s12913-017-2586-4
An Australian general practice based strategy to improve chronic disease prevention, and its impact on patient reported outcomes: evaluation of the preventive evidence into practice cluster randomised controlled trial
Abstract
Background: Implementing evidence-based chronic disease prevention with a practice-wide population is challenging in primary care.
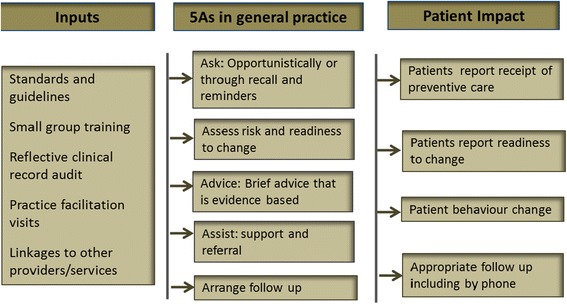
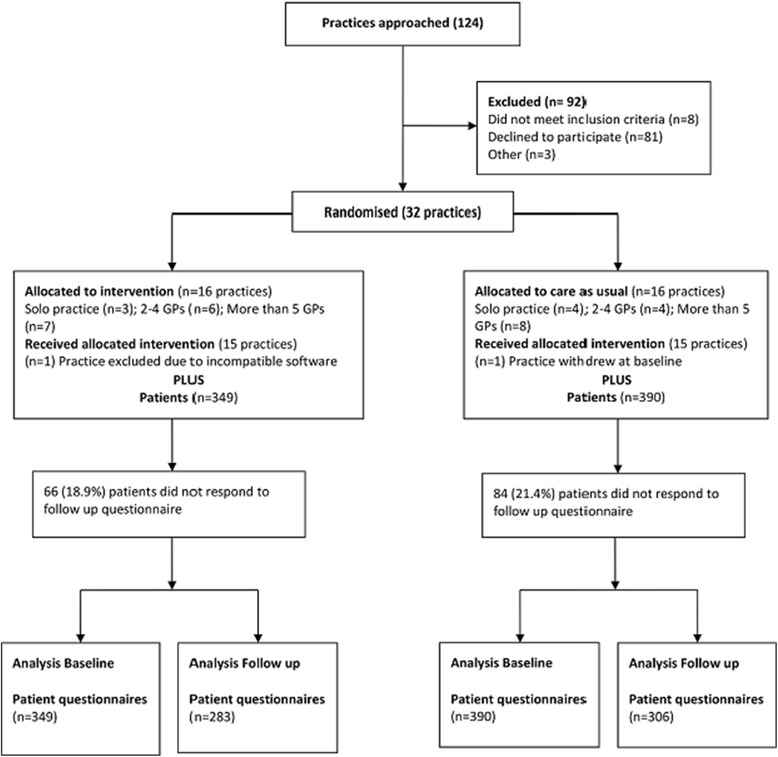
Methods: PEP Intervention practices received education, clinical audit and feedback and practice facilitation. Patients (40‑69 years) without chronic disease from trial and control practices were invited to participate in baseline and 12 month follow up questionnaires. Patient-recalled receipt of GP services and referral, and the proportion of patients at risk were compared over time and between intervention and control groups. Mean difference in BMI, diet and physical activity between baseline and follow up were calculated and compared using a paired t-test. Change in the proportion of patients meeting the definition for physical activity diet and weight risk was calculated using McNemar's test and multilevel analysis was used to determine the effect of the intervention on follow-up scores.
Results: Five hundred eighty nine patients completed both questionnaires. No significant changes were found in the proportion of patients reporting a BP, cholesterol, glucose or weight check in either group. Less than one in six at-risk patients reported receiving lifestyle advice or referral at baseline with little change at follow up. More intervention patients reported attempts to improve their diet and reduce weight. Mean score improved for diet in the intervention group (p = 0.04) but self-reported BMI and PA risk did not significantly change in either group. There was no significant change in the proportion of patients who reported being at-risk for diet, PA or weight, and no changes in PA, diet and BMI in multilevel linear regression adjusted for patient age, sex, practice size and state. There was good fidelity to the intervention but practices varied in their capacity to address changes.
Conclusions: The lack of measurable effect within this trial may be attributable to the complexities around behaviour change and/or system change. This trial highlights some of the challenges in providing suitable chronic disease preventive interventions which are both scalable to whole practice populations and meet the needs of diverse practice structures.
Trial registration: Australian and New Zealand Clinical Trials Registry (ANZCTR): ACTRN12612000578808 (29/5/2012). This trial registration is retrospective as our first patient returned their consent on the 21/5/2012. Patient recruitment was ongoing until 31/10/2012.
Keywords: Cardiovascular disease; Delivery of health care; Evidence based medicine; Primary health care, Family practice, Primary prevention; Quality improvement; practice guidelines.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the National Research and Evaluation Ethics Committee of the RACGP (NREEC 10–002), and ratified by the Institutional Ethics Committees of participating universities. All participants provided full informed written consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Agency for Health Research and Quality: The Guide to Clinical Preventive Services. Recommendations of the U.S. Preventive Services Task Force. Rockville: Agency for Healthcare Research and Quality (US); 2014. - PubMed
-
- National Health Priority Action Council . National Chronic Disease Strategy. Canberra: Australian Government Department of Health and Ageing; 2006.
-
- Royal Australian College of General Practitioners: Putting prevention into practice. Guidelines for the implementation of prevention in the general practice setting. 2nd ed. Melbourne: RACGP; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
