

Validation of Postinduction Curie Scores in High-Risk Neuroblastoma: A Children's Oncology Group and SIOPEN Group Report on SIOPEN/HR-NBL1
- PMID: 28887399
- PMCID: PMC5868501
- DOI: 10.2967/jnumed.117.195883
Validation of Postinduction Curie Scores in High-Risk Neuroblastoma: A Children's Oncology Group and SIOPEN Group Report on SIOPEN/HR-NBL1
Abstract
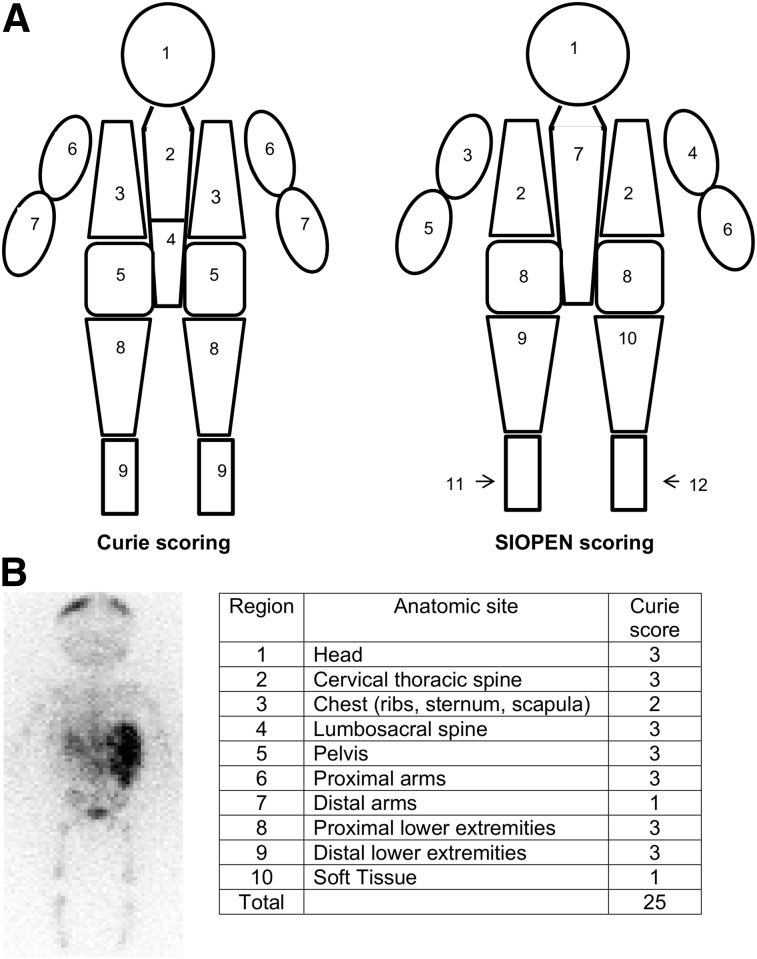
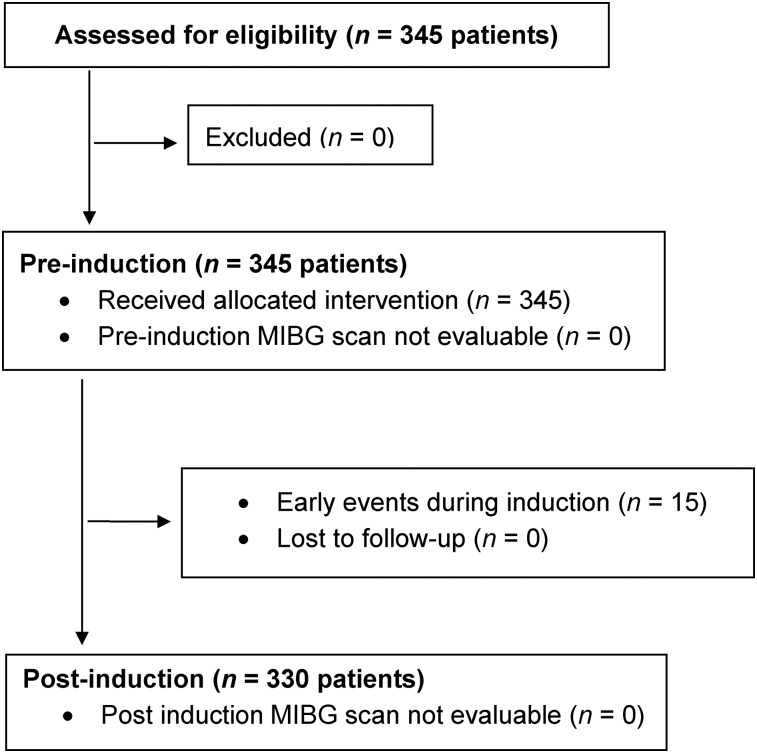
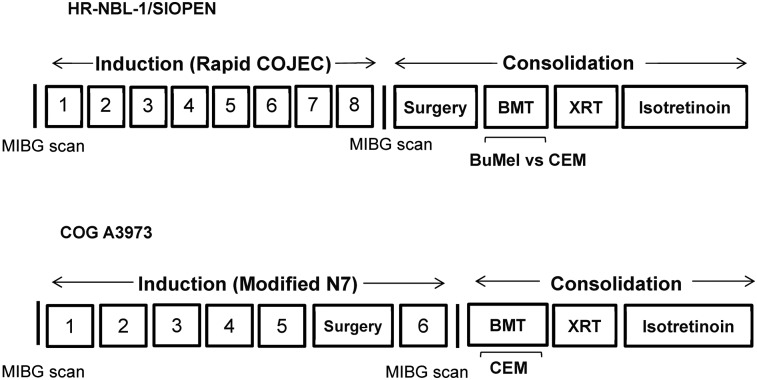
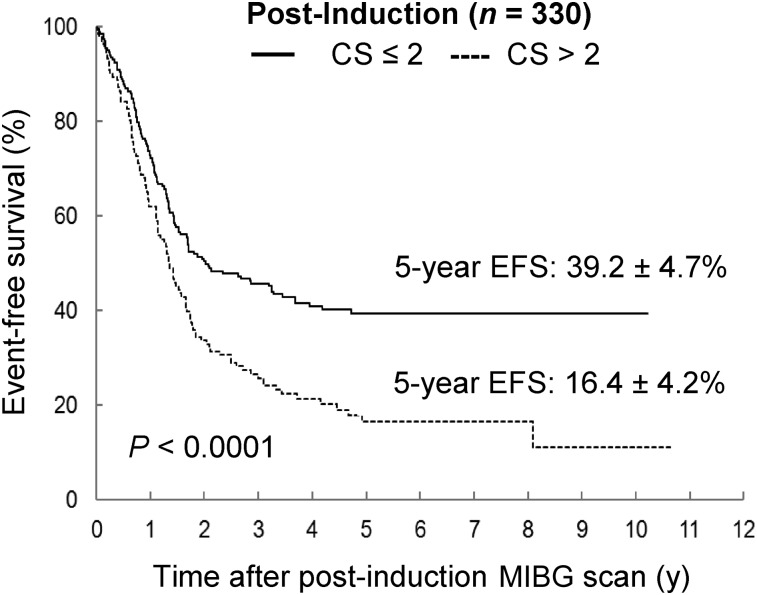
A semiquantitative 123I-metaiodobenzylguanidine (123I-MIBG) scoring method (the Curie score, or CS) was previously examined in the Children's Oncology Group (COG) high-risk neuroblastoma trial, COG A3973, with a postinduction CS of more than 2 being associated with poor event-free survival (EFS). The validation of the CS in an independent dataset, International Society of Paediatric Oncology European Neuroblastoma/High-Risk Neuroblastoma 1 (SIOPEN/HR-NBL1), is now reported. Methods: A retrospective analysis of 123I-MIBG scans obtained from patients who had been prospectively enrolled in SIOPEN/HR-NBL1 was performed. All patients exhibited 123I-MIBG-avid, International Neuroblastoma Staging System stage 4 neuroblastoma. 123I-MIBG scans were evaluated at 2 time points, diagnosis (n = 345) and postinduction (n = 330), before consolidation myeloablative therapy. Scans of 10 anatomic regions were evaluated, with each region being scored 0-3 on the basis of disease extent and a cumulative CS generated. Cut points for outcome analysis were identified by Youden methodology. CSs from patients enrolled in COG A3973 were used for comparison. Results: The optimal cut point for CS at diagnosis was 12 in SIOPEN/HR-NBL1, with a significant outcome difference by CS noted (5-y EFS, 43.0% ± 5.7% [CS ≤ 12] vs. 21.4% ± 3.6% [CS > 12], P < 0.0001). The optimal CS cut point after induction was 2 in SIOPEN/HR-NBL1, with a postinduction CS of more than 2 being associated with an inferior outcome (5-y EFS, 39.2% ± 4.7% [CS ≤ 2] vs. 16.4% ± 4.2% [CS > 2], P < 0.0001). The postinduction CS maintained independent statistical significance in Cox models when adjusted for the covariates of age and MYCN gene copy number. Conclusion: The prognostic significance of postinduction CSs has now been validated in an independent cohort of patients (SIOPEN/HR-NBL1), with a postinduction CS of more than 2 being associated with an inferior outcome in 2 independent large, cooperative group trials.
Keywords: Curie score; MIBG; neuroblastoma.
© 2018 by the Society of Nuclear Medicine and Molecular Imaging.
Figures


References
-
- Ladenstein R, Valteau-Couanet D, Brock P, et al. Randomized trial of prophylactic granulocyte colony-stimulating factor during rapid COJEC induction in pediatric patients with high-risk neuroblastoma: European SIOPEN/HR-NBL-1 study. J Clin Oncol. 2010;28:3516–3524. - PubMed
-
- Ladenstein R, Potschger U, Pearson AD, et al. Busulfan and melphalan versus carboplatin, etoposide, and melphalan as high-dose chemotherapy for high-risk neuroblastoma (SIOPEN/HR-NBL1): an international, randomised, multi-arm, open-label, phase 3 trial. Lancet Oncol. 2017;18:500–514. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous