

doi: 10.2967/jnumed.117.195255.
Epub 2017 Sep 8.
Proposal for a Structured Reporting System for Prostate-Specific Membrane Antigen-Targeted PET Imaging: PSMA-RADS Version 1.0
Affiliations
- PMID: 28887401
- PMCID: PMC6910634
- DOI: 10.2967/jnumed.117.195255
Item in Clipboard
Proposal for a Structured Reporting System for Prostate-Specific Membrane Antigen-Targeted PET Imaging: PSMA-RADS Version 1.0
J Nucl Med.
2018 Mar.
No abstract available
Figures

PSMA-RADS-1A: whole-body maximum-intensity-projection image of patient with biochemically recurrent PCa imaged with 18F-DCFPyL. No sites of abnormal uptake can be appreciated. Normal biodistribution of agent is seen, including uptake in lacrimal glands, salivary glands, liver, spleen, kidneys, and small bowel. In addition, radiotracer is seen being excreted within urinary tract.
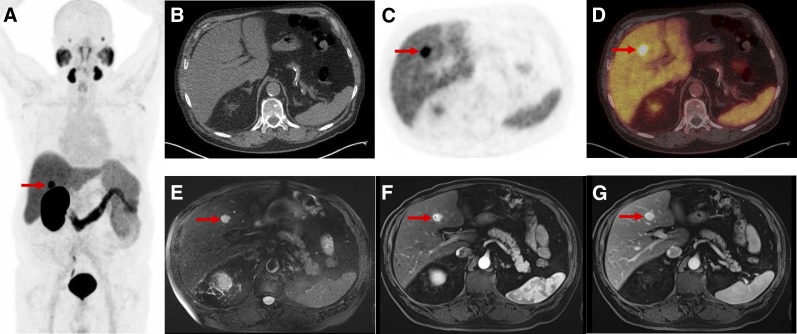
PSMA-RADS-1B: images of patient with biochemically recurrent PCa found to have hepatic hemangioma on both18F-DCFPyL PET/CT and MRI. (A) Maximum-intensity-projection 18F-DCFPyL PET image shows intense focus projecting over right lobe of liver. (Patient had left nephrectomy for remote history of renal cell carcinoma.) Very small lymph nodes in retroperitoneum that were thought to represent recurrent PCa are not well seen. (B–D) Axial CT (B), axial 18F-DCFPyL PET (C), and axial 18F-DCFPyL PET/CT (D) images through liver corroborate that intense focus is in segment IVB (arrows) and has no anatomic correlate on CT. (E–F) T2 fat-saturation (E), T1 fat-saturation enhanced (20 s after 11.5-mL gadobutrol injection) (F), and T1 fat-saturation enhanced (70 s after 11.5-mL gadobutrol injection) images from subsequent MRI (G) show homogeneous T2 bright lesion in segment IVB at location of PET abnormality, with brisk peripheral contrast uptake on earlier image and complete fill-in on later image. No restricted diffusion was evident. MRI findings are typical of hepatic hemangioma.
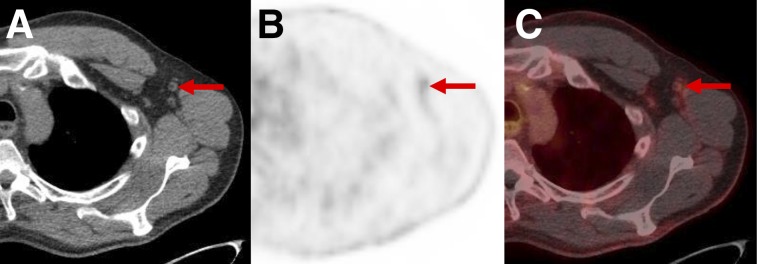
PSMA-RADS-2: likely benign lymph nodes with uptake in patient with biochemically recurrent PCa. Axial CT (A), axial 18F-DCFPyL PET (B), and axial 18F-DCFPyL PET/CT (C) images show mild uptake in multiple axillary lymph nodes. Such findings in axillae (and lung hila and mediastinum) indicate chronic inflammatory process and are not overtly suggestive of PCa in setting of biochemical recurrence.
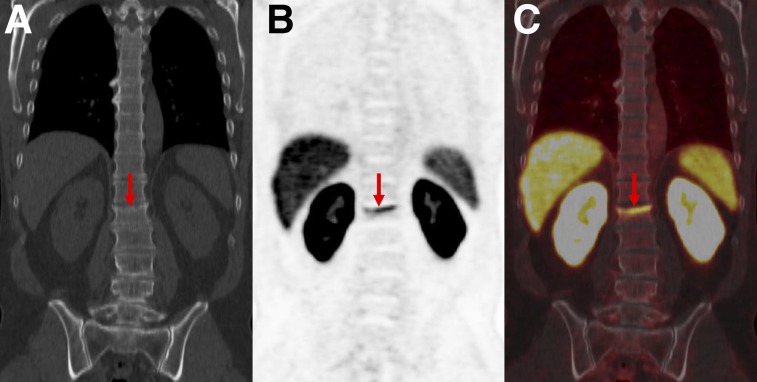
PSMA-RADS-2: likely benign skeletal finding with uptake in patient with biochemically recurrent PCa. Patient was an avid bicyclist and had experienced several episodes of minor trauma over the years, including a recent back injury. Coronal CT (A), coronal 18F-DCFPyL PET (B), and coronal 18F-DCFPyL PET/CT images (C) show slightly depressed L1 superior endplate with smooth, linear uptake (arrows). This uptake can occur in healing fractures and generally does not indicate disease. We categorized this patient as PSMA-RADS-2 instead of PSMA-RADS-1B because in rare circumstances uptake in such a location may obscure uptake from PCa.
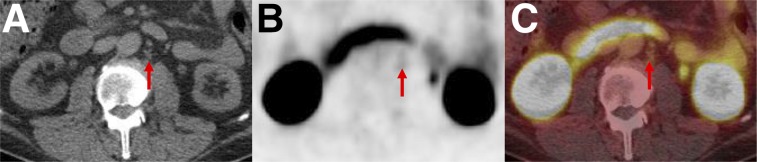
PSMA-RADS-3A: equivocal uptake in several retroperitoneal lymph nodes of patient with rapidly rising level of prostate-specific antigen and no other evidence of disease. Axial CT (A), axial 18F-DCFPyL PET (B), and axial 18F-DCFPyL PET/CT (C) images show series of small (short-axis diameter, <0.8 cm) left paraaortic lymph nodes (arrows). Degree of uptake is similar to blood pool, leaving this finding indeterminate. Depending on local practice pattern, biopsy of these nodes may be considered (although biopsy of this site is difficult). Follow-up imaging in 3–6 mo may also be considered.
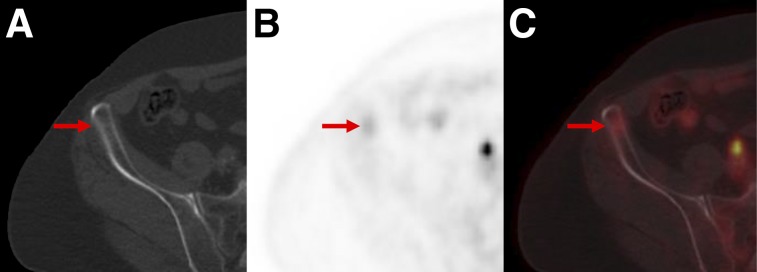
PSMA-RADS-3B: equivocal uptake in bone lesion of patient with recurrent PCa. Axial bone window CT (A), axial 18F-DCFPyL PET (B), and axial 18F-DCFPyL PET/CT (C) images show bone lesion. Pelvic adenopathy was seen on other images. Low-level uptake in anterior right iliac bone (arrows) and lack of anatomic correlates leaves this finding indeterminate for early metastatic disease vs. benign processes such as traumatic changes or small site of fibrous dysplasia. Depending on local practice pattern, biopsy or tumor-protocol MRI may be the preferred follow-up approaches.
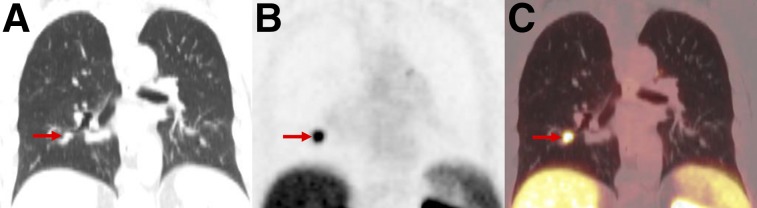
PSMA-RADS-3C: high level of uptake in lung nodule of patient with biochemically recurrent PCa. Coronal CT (A), coronal 18F-DCFPyL PET (B), and coronal 18F-DCFPyL PET/CT (C) images show exceptionally high uptake in right-lower-lobe pulmonary nodule (arrows). Patient’s low prostate-specific antigen level was discordant with this finding. Biopsy of lesion was recommended.

PSMA-RADS-3D: non–radiotracer-avid lung nodule in patient with biochemically recurrent PCa. Axial lung window CT (A), axial 18F-DCFPyL PET (B), and axial 18F-DCFPyL PET/CT (C) images show 1.5-cm right upper lobe nodule without appreciable uptake (arrows). Patient had sites of disease in pelvis to explain his elevated prostate-specific antigen level. Although uptake of PSMA-targeted radiotracers has been described for primary bronchogenic neoplasms, it is unknown what lack of uptake implies about this lung lesion. 18F-FDG PET/CT was recommended as an initial step, with the eventual need for tissue diagnosis being likely.
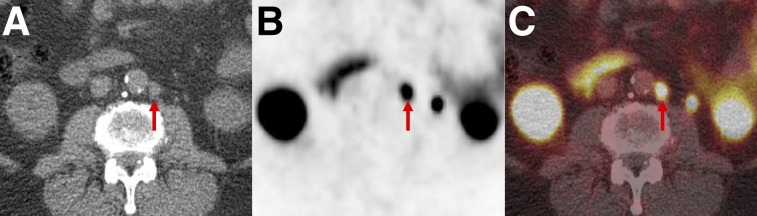
PSMA-RADS-4: radiotracer-avid retroperitoneal lymph node without definitive findings on conventional imaging. Axial CT (A), axial 18F-DCFPyL PET (B), and axial 18F-DCFPyL PET/CT (C) images show a degree of uptake consistent with metastatic PCa (arrows). However, because short-axis diameter of lymph node was 0.7 cm (i.e., <1.0 cm) this node would generally not be considered pathologically enlarged.
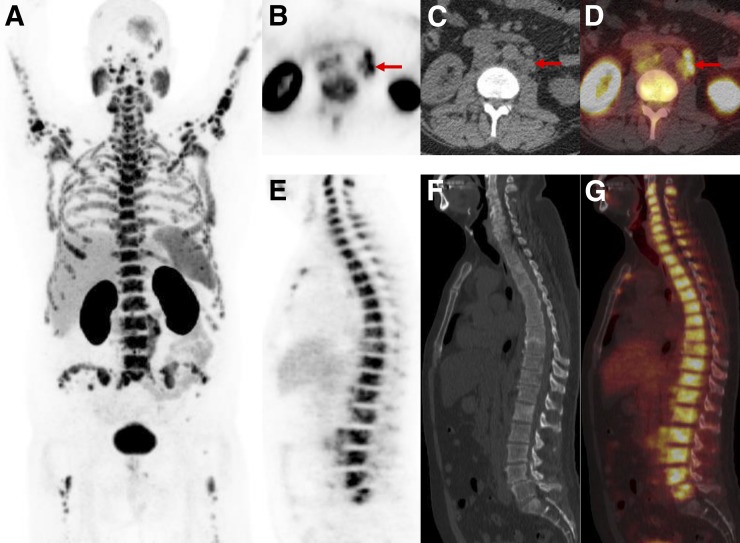
PSMA-RADS-5: images of patient with extensive metastatic PCa. (A) Whole-body maximum-intensity-projection image shows diffuse osseous metastatic disease and retroperitoneal adenopathy. This scan would be categorized as PSMA-RADS-5, and there are also several individual PSMA-RADS-5 lesions. (B–D) Axial CT (B), axial 18F-DCFPyL PET (C), and axial 18F-DCFPyL PET/CT (D) images through retroperitoneum show multiple enlarged lymph nodes (short-axis diameter, >1.0 cm) with intense uptake (arrows). (E–G) Sagittal bone window CT (E), sagittal 18F-DCFPyL PET (F), and sagittal 18F-DCFPyL PET/CT (G) images show diffuse metastatic disease in spine with intense uptake and underlying sclerotic changes in bones. Lack of sacral uptake in F and G is due to previous pelvic radiation therapy.
Comment in
-
Proposed Criteria Positions PSMA PET for the Future.J Nucl Med. 2018 Mar;59(3):466-468. doi: 10.2967/jnumed.117.204057. Epub 2018 Jan 4. J Nucl Med. 2018. PMID: 29301930 No abstract available.
References
-
- Orel SG, Kay N, Reynolds C, Sullivan DC. BI-RADS categorization as a predictor of malignancy. Radiology. 1999;211:845–850. - PubMed
-
- McKee BJ, Regis SM, McKee AB, Flacke S, Wald C. Performance of ACR Lung-RADS in a clinical CT lung screening program. J Am Coll Radiol. 2015;12:273–276. - PubMed
-
- Purysko AS, Remer EM, Coppa CP, Leao Filho HM, Thupili CR, Veniero JC. LI-RADS: a case-based review of the new categorization of liver findings in patients with end-stage liver disease. Radiographics. 2012;32:1977–1995. - PubMed
-
- Tessler FN, Middleton WD, Grant EG, et al. ACR thyroid imaging, reporting and data system (TI-RADS): white Paper of the ACR TI-RADS committee. J Am Coll Radiol. 2017;14:587–595. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous