

Long-term patient reported outcomes following radiation therapy for oropharyngeal cancer: cross-sectional assessment of a prospective symptom survey in patients ≥65 years old
- PMID: 28888224
- PMCID: PMC5591495
- DOI: 10.1186/s13014-017-0878-9
Long-term patient reported outcomes following radiation therapy for oropharyngeal cancer: cross-sectional assessment of a prospective symptom survey in patients ≥65 years old
Erratum in
-
Correction to: Long-term patient reported outcomes following radiation therapy for oropharyngeal cancer: cross-sectional assessment of a prospective symptom survey in patients ≥65 years old.Radiat Oncol. 2017 Nov 23;12(1):186. doi: 10.1186/s13014-017-0921-x. Radiat Oncol. 2017. PMID: 29169353 Free PMC article.
Abstract
Background: Given the potential for older patients to experience exaggerated toxicity and symptoms, this study was performed to characterize patient reported outcomes in older patients following definitive radiation therapy (RT) for oropharyngeal cancer (OPC).
Methods: Cancer-free head and neck cancer survivors (>6 months since treatment completion) were eligible for participation in a questionnaire-based study. Participants completed the MD Anderson Symptom Inventory-Head and Neck module (MDASI-HN). Those patients ≥65 years old at treatment for OPC with definitive RT were included. Individual and overall symptom severity and clinical variables were analyzed.
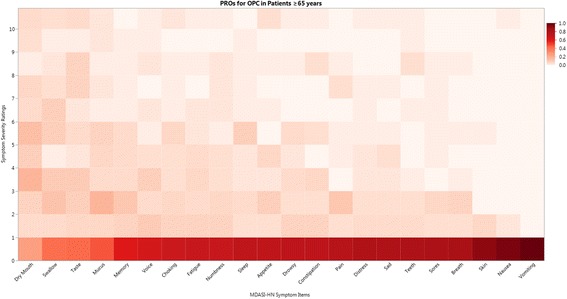
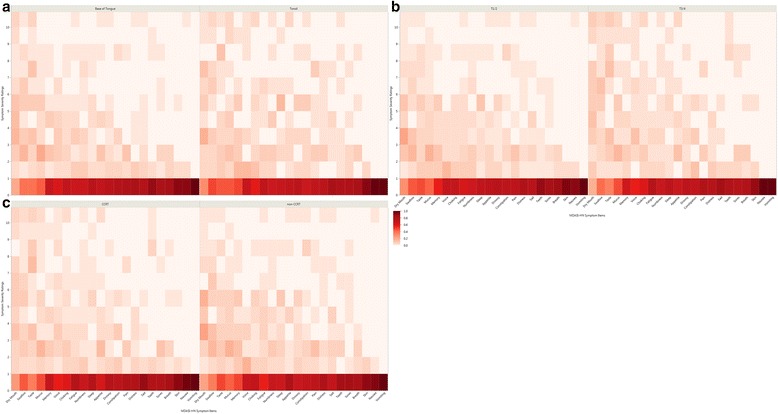
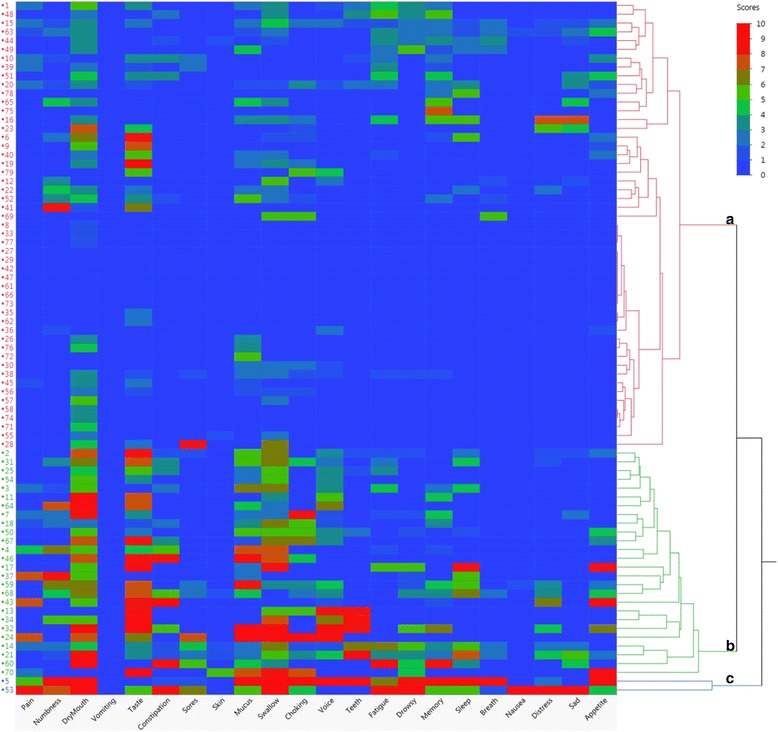
Results: Of the 79 participants analyzed, 82% were male, 95% white, 41% T3/4 disease, 39% RT alone, 27% induction chemotherapy, 52% concurrent, and 18% both, and 96% IMRT. Median age at RT was 71 yrs. (range: 65-85); median time from RT to MDASI-HN was 46 mos. (2/3 > 24 mos.). The top 5 MDASI-HN items rated most severe in terms of mean (±SD) ratings (0-10 scale) were dry mouth (3.48 ± 2.95), taste (2.81 ± 3.29), swallowing (2.59 ± 2.96), mucus in mouth/throat (2.04 ± 2.68), and choking (1.30 ± 2.38) reported at moderate-severe levels (≥5) by 35, 29, 29, 18, and 13%, respectively. Thirty-nine % reported none (0) or no more than mild (1-4) symptoms across all 22 MDASI-HN symptoms items, and 38% had at least one item rated as severe (≥7). Hierarchical cluster analysis resulted in 3 patient groups: 1) ~65% with ranging from none to moderate symptom burden, 2) ~35% with moderate-severe ratings for a subset of classically RT-related symptoms (e.g. dry mouth, mucus, swallowing) and 3) 2 pts. with severe ratings of most items.
Conclusions: The overall long-term symptom burden seen in this older OPC cohort treated with modern standard therapy was largely favorable, yet a higher symptom group (~35%) with a distinct pattern of mostly local and classically RT-related symptoms was identified.
Keywords: Oropharynx; Patient reported outcomes; Symptoms.
Conflict of interest statement
Ethics approval and consent to participate
MDACC Protocol ID #: DR09–0891.
Protocol Title: Prospective Data Collection of Symptom Burden in Patients Previously Treated for Head and Neck Cancer.
Official IRB Approval Date: 04/23/2010.
Official Activation Date: 07/15/2010.
It was noted that the protocol, informed consent documents (ICDs) and/or the Waivers of ICD and Authorization are satisfactory and in compliance with federal and institutional guidelines. It was also noted that risks to human subjects are minimal and that confidentiality of records will be maintained.
Consent for publication
Not applicable.
Competing interests
Dr. Fuller has received direct industry grant funding and speaker travel from Elekta AB for unrelated technical projects.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Zumsteg ZS, Lok BH, Ho AS, Drill E, Zhang Z, Riaz N, et al. The toxicity and efficacy of concomitant chemoradiotherapy in patients aged 70 years and older with oropharyngeal carcinoma in the intensity-modulated radiotherapy era. Cancer. 2017;123(8):1345–53. doi: 10.1002/cncr.30495. - DOI - PMC - PubMed
-
- Ludbrook JJS, Truong PT, MacNeil MV, Lesperance M, Webber A, Joe H, et al. Do age and comorbidity impact treatment allocation and outcomes in limited stage small-cell lung cancer? A community-based population analysis. Int J Radiat Oncol Biol Phys. 2003;55:1321–1330. doi: 10.1016/S0360-3016(02)04576-5. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
