

Fatal Anaphylaxis: Mortality Rate and Risk Factors
- PMID: 28888247
- PMCID: PMC5589409
- DOI: 10.1016/j.jaip.2017.06.031
Fatal Anaphylaxis: Mortality Rate and Risk Factors
Abstract
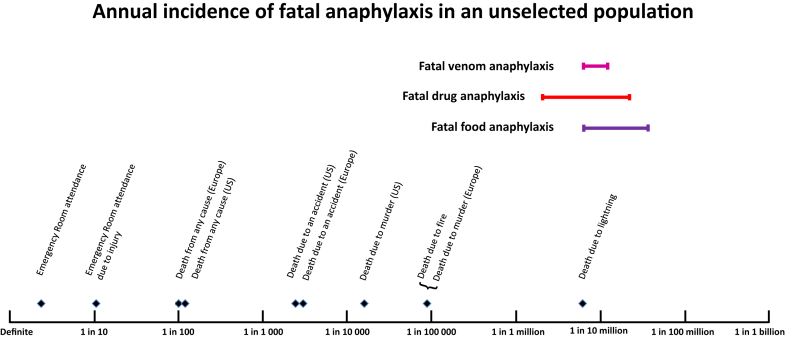
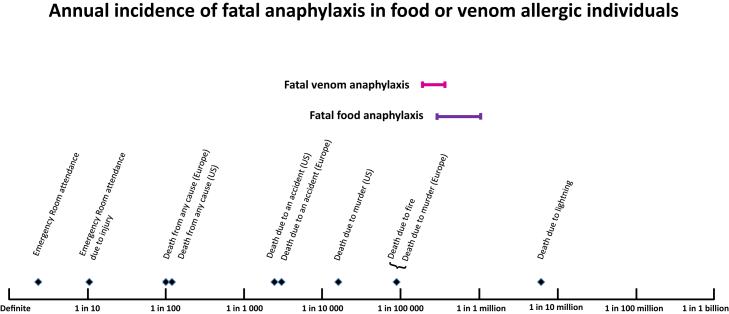
Up to 5% of the US population has suffered anaphylaxis. Fatal outcome is rare, such that even for people with known venom or food allergy, fatal anaphylaxis constitutes less than 1% of total mortality risk. The incidence of fatal anaphylaxis has not increased in line with hospital admissions for anaphylaxis. Fatal drug anaphylaxis may be increasing, but rates of fatal anaphylaxis to venom and food are stable. Risk factors for fatal anaphylaxis vary according to cause. For fatal drug anaphylaxis, previous cardiovascular morbidity and older age are risk factors, with beta-lactam antibiotics, general anesthetic agents, and radiocontrast injections the commonest triggers. Fatal food anaphylaxis most commonly occurs during the second and third decades. Delayed epinephrine administration is a risk factor; common triggers are nuts, seafood, and in children, milk. For fatal venom anaphylaxis, risk factors include middle age, male sex, white race, cardiovascular disease, and possibly mastocytosis; insect triggers vary by region. Upright posture is a feature of fatal anaphylaxis to both food and venom. The rarity of fatal anaphylaxis and the significant quality of life impact of allergic conditions suggest that quality of life impairment should be a key consideration when making treatment decisions in patients at risk for anaphylaxis.
Keywords: Anaphylaxis; Drug allergy; Food allergy; Insect sting; Mortality.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wood R.A., Camargo C.A., Jr., Lieberman P., Sampson H.A., Schwartz L.B., Zitt M. Anaphylaxis in America: the prevalence and characteristics of anaphylaxis in the United States. J Allergy Clin Immunol. 2014;133:461–467. - PubMed
-
- Rona R.J., Keil T., Summers C., Gislason D., Zuidmeer L., Sodergren E. The prevalence of food allergy: a meta-analysis. J Allergy Clin Immunol. 2007;120:638–646. - PubMed
-
- Branum A.M., Lukacs S.L. Food allergy among children in the United States. Pediatrics. 2009;124:1549–1555. - PubMed
-
- Tanno L.K., Ganem F., Demoly P., Toscano C.M., Bierrenbach A.L. Undernotification of anaphylaxis deaths in Brazil due to difficult coding under the ICD-10. Allergy. 2012;67:783–789. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
