

New York Heart Association class and the survival benefit from primary prevention implantable cardioverter defibrillators: A pooled analysis of 4 randomized controlled trials
- PMID: 28888266
- PMCID: PMC5657554
- DOI: 10.1016/j.ahj.2017.06.002
New York Heart Association class and the survival benefit from primary prevention implantable cardioverter defibrillators: A pooled analysis of 4 randomized controlled trials
Abstract
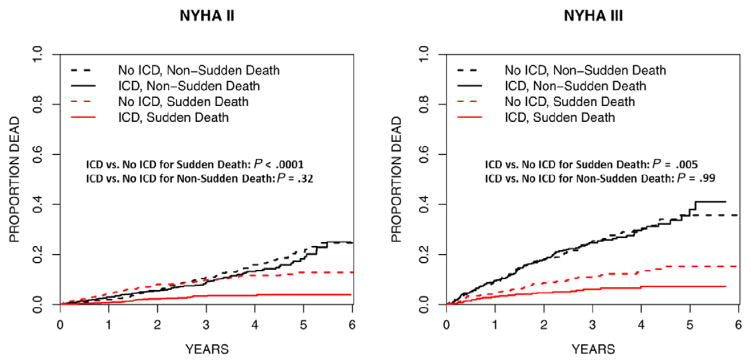
Background: Primary prevention implantable cardioverter defibrillator (ICD) reduce all-cause mortality by reducing sudden cardiac death. There are conflicting data regarding whether patients with more advanced heart failure derive ICD benefit owing to the competing risk of nonsudden death.
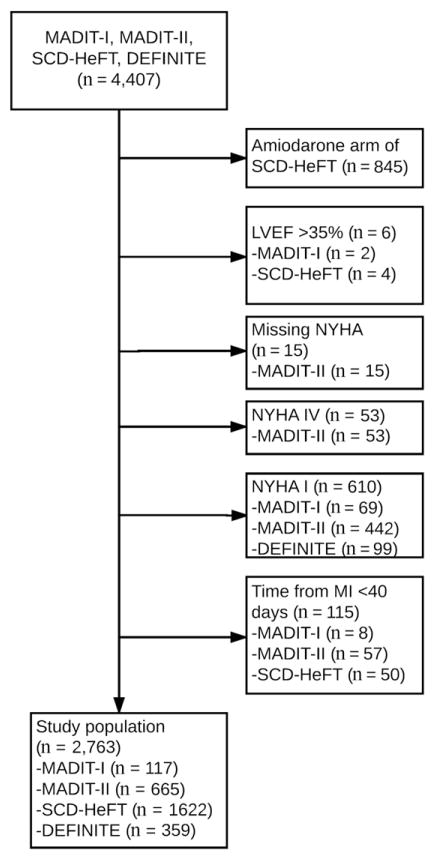
Methods: We performed a patient-level meta-analysis of New York Heart Association (NYHA) class II/III heart failure patients (left ventricular ejection fraction ≤35%) from 4 primary prevention ICD trials (MADIT-I, MADIT-II, DEFINITE, SCD-HeFT). Bayesian-Weibull survival regression models were used to assess the impact of NYHA class on the relationship between ICD use and mortality.
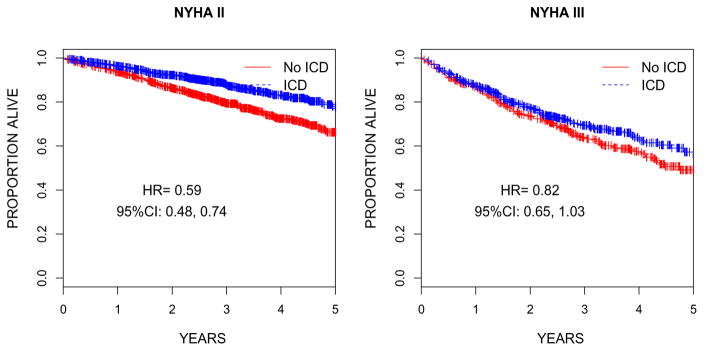
Results: Of the 2,763 patients who met study criteria, 68% (n=1,867) were NYHA II and 52% (n=1,435) were randomized to an ICD. In a multivariable model including all study patients, the ICD reduced mortality (hazard ratio [HR] 0.65, 95% posterior credibility interval [PCI]) 0.40-0.99). The interaction between NYHA class and the ICD on mortality was significant (posterior probability of no interaction=.036). In models including an interaction term for the NYHA class and ICD, the ICD reduced mortality among NYHA class II patients (HR 0.55, PCI 0.35-0.85), and the point estimate suggested reduced mortality in NYHA class III patients (HR 0.76, PCI 0.48-1.24), although this was not statistically significant.
Conclusions: Primary prevention ICDs reduce mortality in NYHA class II patients and trend toward reducing mortality in the heterogeneous group of NYHA class III patients. Improved risk stratification tools are required to guide patient selection and shared decision making among NYHA class III primary prevention ICD candidates.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–51. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, et al. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999;341:1882–90. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med. 1996;335:1933–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
