

The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE)
- PMID: 28890157
- PMCID: PMC5798235
- DOI: 10.1016/S0140-6736(17)31610-0
The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE)
Abstract
Background: Survivors of childhood cancer develop early and severe chronic health conditions (CHCs). A quantitative landscape of morbidity of survivors, however, has not been described. We aimed to describe the cumulative burden of curative cancer therapy in a clinically assessed ageing population of long-term survivors of childhood cancer.
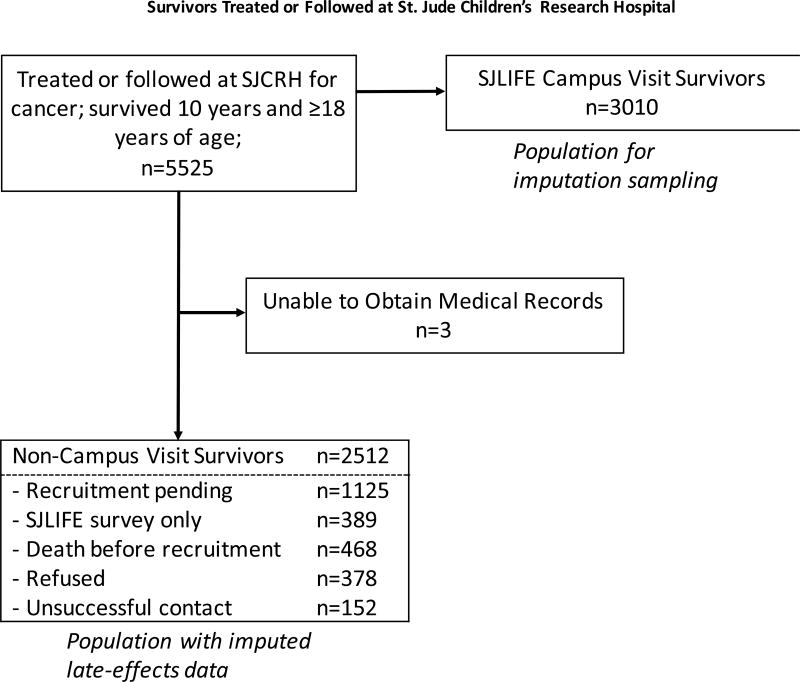
Methods: The St Jude Lifetime Cohort Study (SJLIFE) retrospectively collected data on CHCs in all patients treated for childhood cancer at the St Jude Children's Research Hospital who survived 10 years or longer from initial diagnosis and were 18 years or older as of June 30, 2015. Age-matched and sex-frequency-matched community controls were used for comparison. 21 treatment exposure variables were included in the analysis, with data abstracted from medical records. 168 CHCs for all participants were graded for severity using a modified Common Terminology Criteria of Adverse Events. Multiple imputation with predictive mean matching was used for missing occurrences and grades of CHCs in the survivors who were not clinically evaluable. Mean cumulative count was used for descriptive cumulative burden analysis and marked-point-process regression was used for inferential cumulative burden analysis.
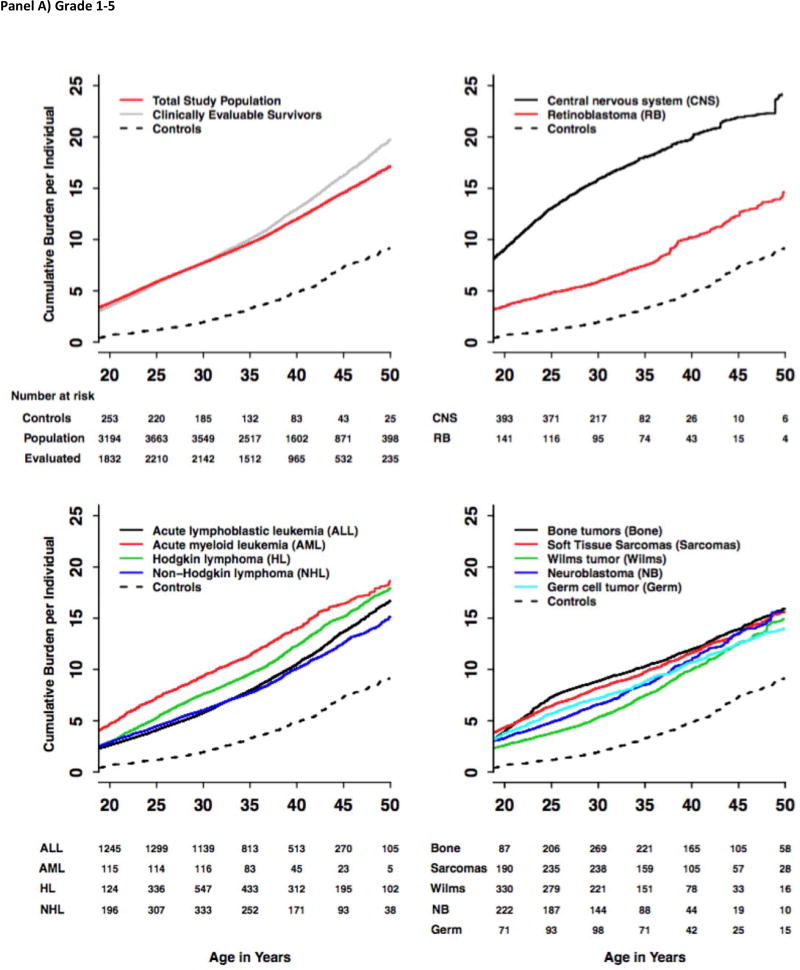
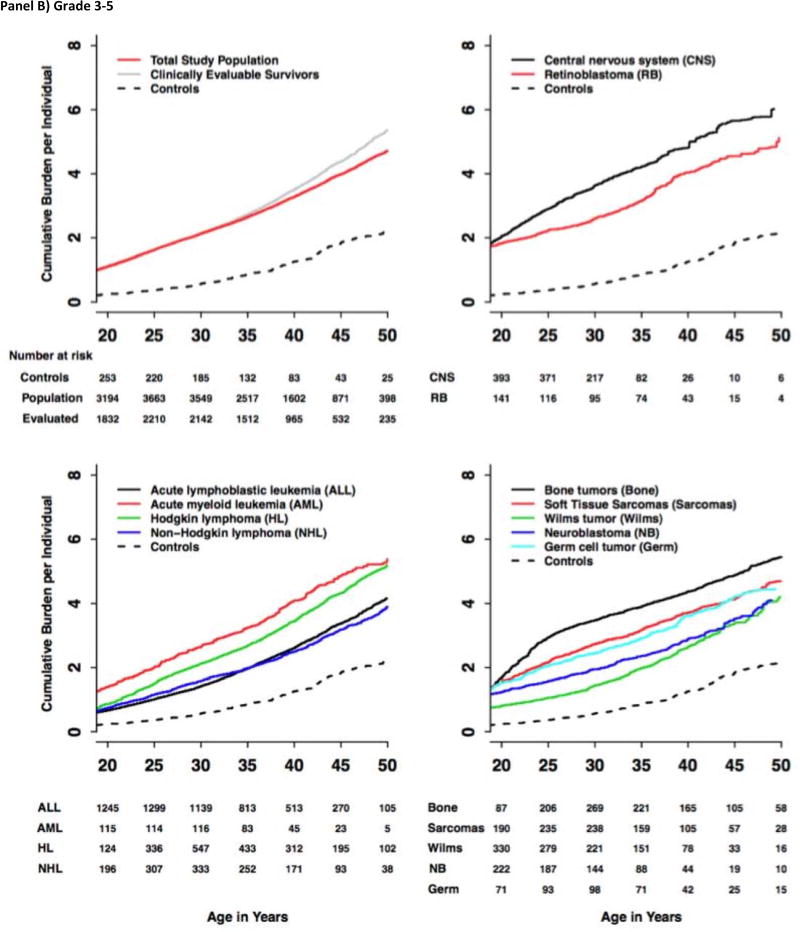
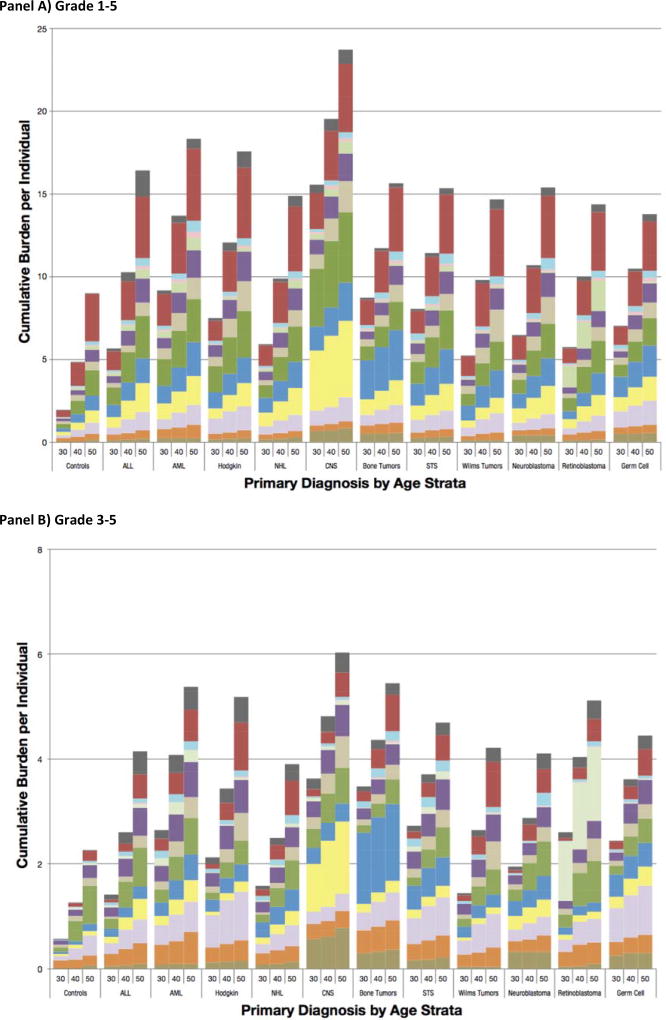
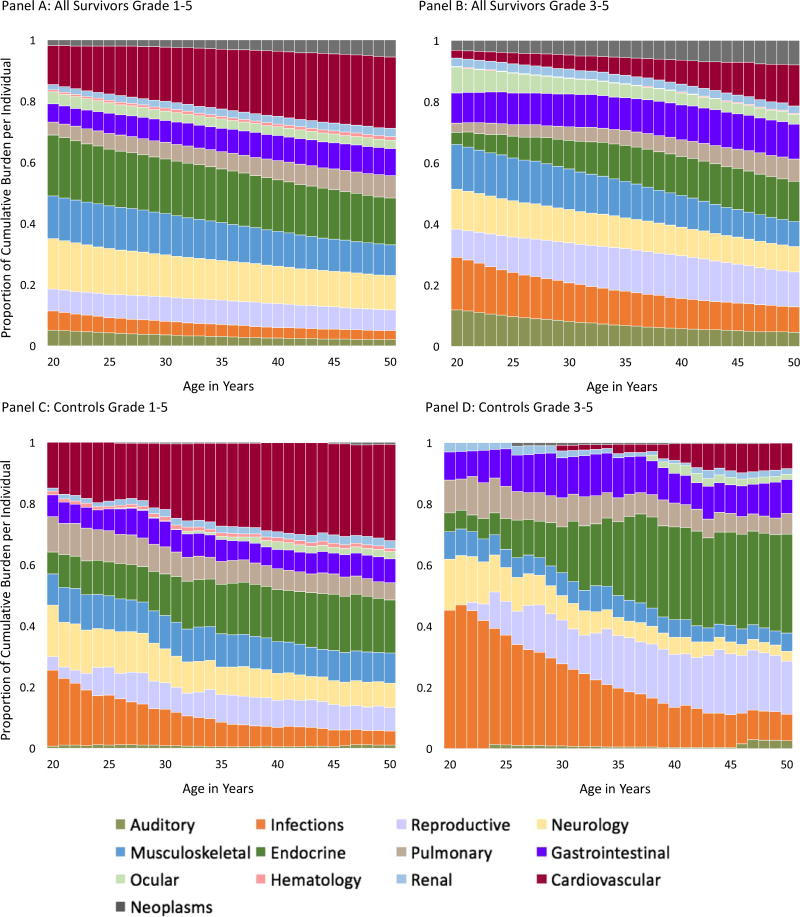
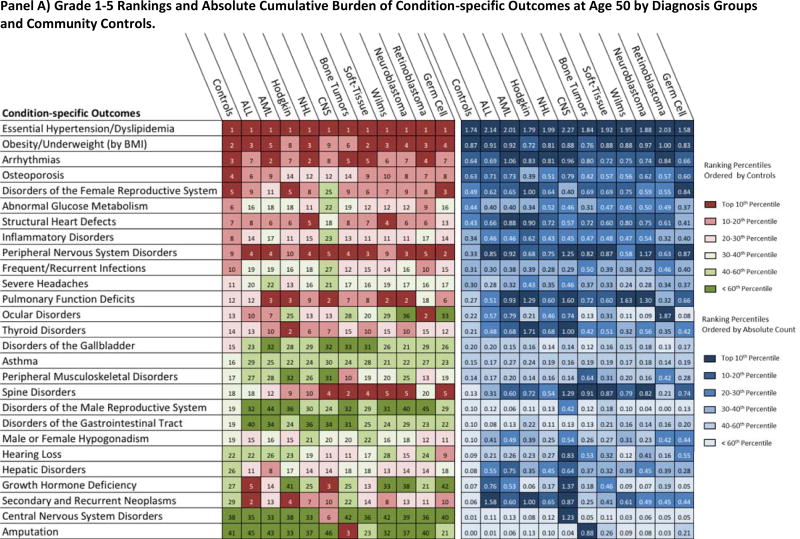
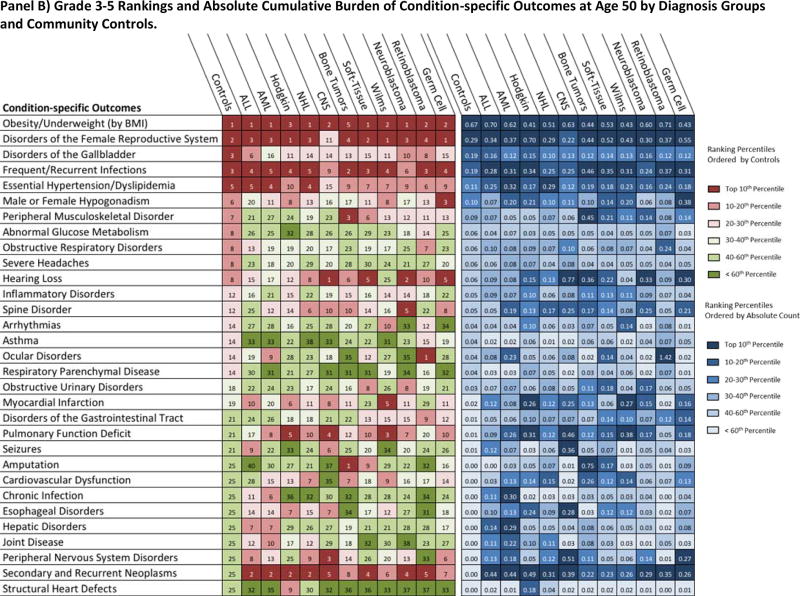
Findings: Of 5522 patients treated for childhood cancer at St Jude Children's Research Hospital who had complete records, survived 10 years or longer, and were 18 years or older at time of study, 3010 (54·5%) were alive, had enrolled, and had had prospective clinical assessment. 2512 (45·5%) of the 5522 patients were not clinically evaluable. The cumulative incidence of CHCs at age 50 years was 99·9% (95% CI 99·9-99·9) for grade 1-5 CHCs and 96·0% (95% CI 95·3-96·8%) for grade 3-5 CHCs. By age 50 years, a survivor had experienced, on average, 17·1 (95% CI 16·2-18·1) CHCs of any grade, of which 4·7 (4·6-4·9) were CHCs of grade 3-5. The cumulative burden in matched community controls of grade 1-5 CHCs was 9·2 (95% CI 7·9-10·6; p<0·0001 vs total study population) and of grade 3-5 CHCs was 2·3 (1·9-2·7, p<0·0001 vs total study population). Second neoplasms, spinal disorders, and pulmonary disease were major contributors to the excess total cumulative burden. Notable heterogeneity in the distribution of CHC burden in survivors with differing primary cancer diagnoses was observed. The cumulative burden of grade 1-5 CHCs at age 50 years was highest in survivors of CNS malignancies (24·2 [95% CI 20·9-27·5]) and lowest in survivors of germ cell tumours (14·0 [11·5-16·6]). Multivariable analyses showed that older age at diagnosis, treatment era, and higher doses of brain and chest radiation are significantly associated with a greater cumulative burden and severity of CHCs.
Interpretation: The burden of CHCs in survivors of childhood cancer is substantial and highly variable. Our assessment of total cumulative burden in survivors of paediatric cancer, with detailed characterisation of long-term CHCs, provide data to better inform future clinical guidelines, research investigations, and health services planning for this vulnerable, medically complex population.
Funding: The US National Cancer Institute, St Baldrick's Foundation, and the American Lebanese Syrian Associated Charities.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Childhood cancer: the long-term costs of cure.Lancet. 2017 Dec 9;390(10112):2530-2531. doi: 10.1016/S0140-6736(17)31755-5. Epub 2017 Sep 8. Lancet. 2017. PMID: 28890158 No abstract available.
-
Health-care delivery for long-term survivors of childhood cancer.Lancet. 2017 Dec 9;390(10112):2545. doi: 10.1016/S0140-6736(17)33081-7. Epub 2017 Dec 8. Lancet. 2017. PMID: 29231830 No abstract available.
-
Late effects of childhood cancer.Lancet. 2018 May 5;391(10132):1772. doi: 10.1016/S0140-6736(18)30572-5. Lancet. 2018. PMID: 29739563 No abstract available.
-
Late effects of childhood cancer - Authors' reply.Lancet. 2018 May 5;391(10132):1772-1773. doi: 10.1016/S0140-6736(18)30569-5. Lancet. 2018. PMID: 29739564 No abstract available.
-
Re: The Cumulative Burden of Surviving Childhood Cancer: An Initial Report from the St Jude Lifetime Cohort Study (SJLIFE).J Urol. 2018 Jun;199(6):1386-1389. doi: 10.1016/j.juro.2018.03.060. Epub 2018 Mar 20. J Urol. 2018. PMID: 29783574 No abstract available.
References
-
- Howlader NNA, Krapcho M, et al. SEER Cancer Statistics Review (CSR), 1975–2012. [accessed August 1, 2016];2015 http://seer.cancer.gov/csr/1975_2012/
-
- Winther JF, Kenborg L, Byrne J, et al. Childhood cancer survivor cohorts in Europe. Acta Oncol. 2015;54(5):655–68. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
