

Dominant hand, non-dominant hand, or both? The effect of pre-training in hand-eye coordination upon the learning curve of laparoscopic intra-corporeal knot tying
- PMID: 28890675
- PMCID: PMC5570794
- DOI: 10.1186/s10397-017-1015-3
Dominant hand, non-dominant hand, or both? The effect of pre-training in hand-eye coordination upon the learning curve of laparoscopic intra-corporeal knot tying
Abstract
Background: Training of basic laparoscopic psychomotor skills improves both acquisition and retention of more advanced laparoscopic tasks, such as laparoscopic intra-corporeal knot tying (LICK). This randomized controlled trial (RCT) was performed to evaluate the effect of different pre-training programs in hand-eye coordination (HEC) upon the learning curve of LICK.
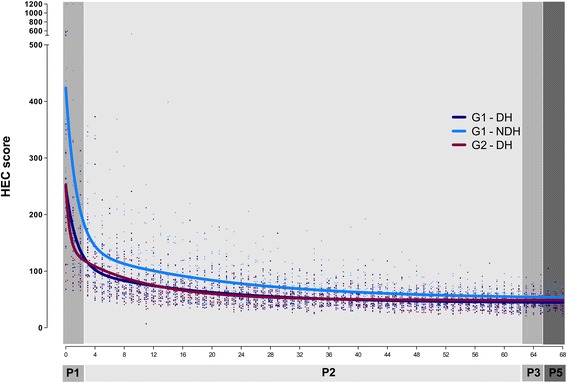
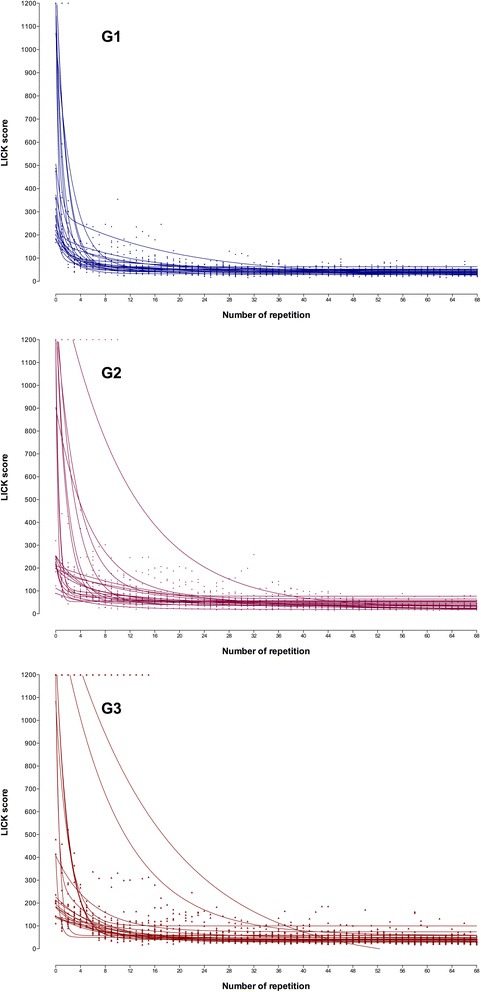
Results: The study was performed in a private center in Asunción, Paraguay, by 60 residents/specialists in gynaecology with no experience in laparoscopic surgery. Participants were allocated in three groups. In phase 1, a baseline test was performed (T1, three repetitions). In phase 2, participants underwent different training programs for HEC (60 repetitions): G1 with both the dominant hand (DH) and the non-dominant hand (NDH), G2 with the DH only, G3 none. In phase 3, a post HEC/pre LICK training test was performed (T2, three repetitions). In phase 4, participants underwent a standardized training program for LICK (60 repetitions). In phase 5, a final test was performed (T3, three repetitions). The score was based on the time taken for task completion system. The scores were plotted and non-linear regression models were used to fit the learning curves to one- and two-phase exponential decay models for each participant (individual curves) and for each group (group curves). For both HEC and LICK, the group learning curves fitted better to the two-phase exponential decay model. For HEC with the DH, G1 and G2 started from a similar point, but G1 reached a lower plateau at a higher speed. In G1, the DH curve started from a lower point than the NDH curve, but both curves reached a similar plateau at comparable speeds. For LICK, all groups started from a similar point, but immediately after HEC training and before LICK training, G1 scored better than the others. All groups reached a similar plateau but with a different decay, G1 reaching this plateau faster than the others groups.
Conclusions: This study demonstrates that pre-training in HEC with both the DH and the NDH shortens the LICK learning curve.
Keywords: Hand-eye coordination; Intra-corporeal knot tying; Laparoscopy; Learning curve; Training.
Conflict of interest statement
Ethics approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


Similar articles
-
A randomized control trial to evaluate the importance of pre-training basic laparoscopic psychomotor skills upon the learning curve of laparoscopic intra-corporeal knot tying.Gynecol Surg. 2017;14(1):29. doi: 10.1186/s10397-017-1031-3. Epub 2017 Dec 20. Gynecol Surg. 2017. PMID: 29290752 Free PMC article.
-
Learning surgical knot tying and suturing technique - effects of different forms of training in a controlled randomized trial with dental students.GMS J Med Educ. 2023 Jun 15;40(4):Doc48. doi: 10.3205/zma001630. eCollection 2023. GMS J Med Educ. 2023. PMID: 37560044 Free PMC article. Clinical Trial.
-
Retention of laparoscopic psychomotor skills after a structured training program depends on the quality of the training and on the complexity of the task.Gynecol Surg. 2016;13(4):395-402. doi: 10.1007/s10397-016-0962-4. Epub 2016 Jul 16. Gynecol Surg. 2016. PMID: 28003800 Free PMC article.
-
Sequential learning of psychomotor and visuospatial skills for laparoscopic suturing and knot tying-a randomized controlled trial "The Shoebox Study" DRKS00008668.Langenbecks Arch Surg. 2016 Sep;401(6):893-901. doi: 10.1007/s00423-016-1421-4. Epub 2016 Apr 7. Langenbecks Arch Surg. 2016. PMID: 27055853 Clinical Trial.
-
Intracorporal knot tying techniques - which is the right one?J Pediatr Surg. 2017 Apr;52(4):633-638. doi: 10.1016/j.jpedsurg.2016.11.049. Epub 2016 Dec 20. J Pediatr Surg. 2017. PMID: 28017412
Cited by
-
A randomized control trial to evaluate the importance of pre-training basic laparoscopic psychomotor skills upon the learning curve of laparoscopic intra-corporeal knot tying.Gynecol Surg. 2017;14(1):29. doi: 10.1186/s10397-017-1031-3. Epub 2017 Dec 20. Gynecol Surg. 2017. PMID: 29290752 Free PMC article.
-
Using Intraoperative Recordings to Evaluate Surgical Technique and Performance in Mastoidectomy.JAMA Otolaryngol Head Neck Surg. 2020 Oct 1;146(10):893-899. doi: 10.1001/jamaoto.2020.2063. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 32780790 Free PMC article.
-
Simulation and Training of Gynaecological Skills.Facts Views Vis Obgyn. 2018 Mar;10(1):21-27. Facts Views Vis Obgyn. 2018. PMID: 30510664 Free PMC article.
-
A haptic laparoscopic trainer based on affine velocity analysis: engineering and preliminary results.BMC Surg. 2021 Mar 18;21(1):139. doi: 10.1186/s12893-021-01128-z. BMC Surg. 2021. PMID: 33736639 Free PMC article.
-
Learning surgical knot tying and suturing technique - effects of different forms of training in a controlled randomized trial with dental students.GMS J Med Educ. 2023 Jun 15;40(4):Doc48. doi: 10.3205/zma001630. eCollection 2023. GMS J Med Educ. 2023. PMID: 37560044 Free PMC article. Clinical Trial.
References
-
- Campo R, Wattiez A, Tanos V, Di Spiezio SA, Grimbizis G, Wallwiener D, Brucker S, Puga M, Molinas R, O'Donovan P, Deprest J, Van BY, Lissens A, Herrmann A, Tahir M, Benedetto C, Siebert I, Rabischong B, De Wilde RL. Gynaecological endoscopic surgical education and assessment. A diploma programme in gynaecological endoscopic surgery. Eur J Obstet Gynecol Reprod Biol. 2016;199:183–186. doi: 10.1016/j.ejogrb.2016.02.003. - DOI - PubMed
-
- Diesen DL, Erhunmwunsee L, Bennett KM, Ben-David K, Yurcisin B, Ceppa EP, Omotosho PA, Perez A, Pryor A. Effectiveness of laparoscopic computer simulator versus usage of box trainer for endoscopic surgery training of novices. J Surg Educ. 2011;68:282–289. doi: 10.1016/j.jsurg.2011.02.007. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources