

Diagnostic accuracy study of routine echocardiography for bicuspid aortic valve: a retrospective study and meta-analysis
- PMID: 28890873
- PMCID: PMC5582058
- DOI: 10.21037/cdt.2017.05.03
Diagnostic accuracy study of routine echocardiography for bicuspid aortic valve: a retrospective study and meta-analysis
Abstract
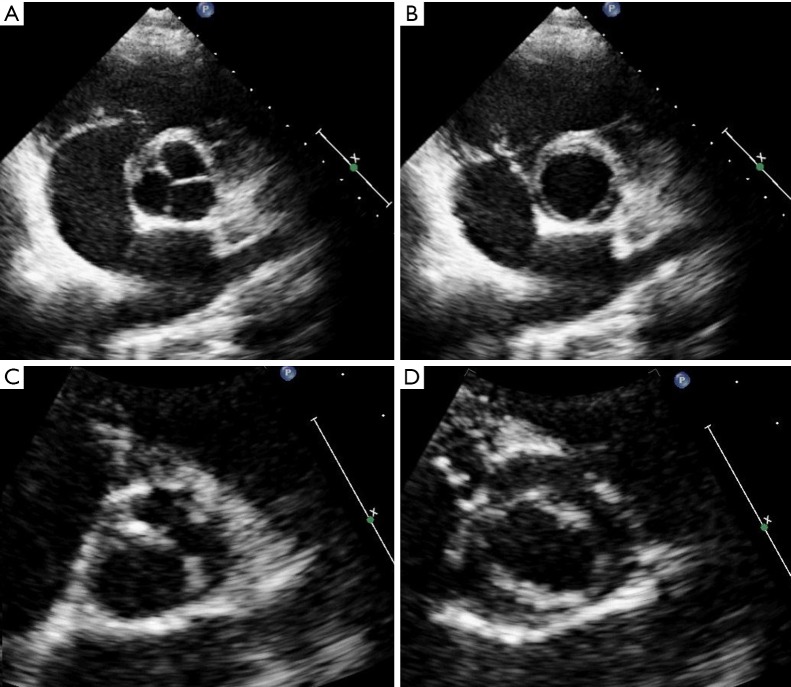
Background: Transthoracic echocardiography (TTE) is the standard procedure to distinguish tricuspid aortic valve (TAV) from bicuspid aortic valve (BAV). Published studies assessed the accuracy of TTE for BAV under ideal conditions. Conversely, we aimed at assessing accuracy of TTE for BAV under routine conditions.
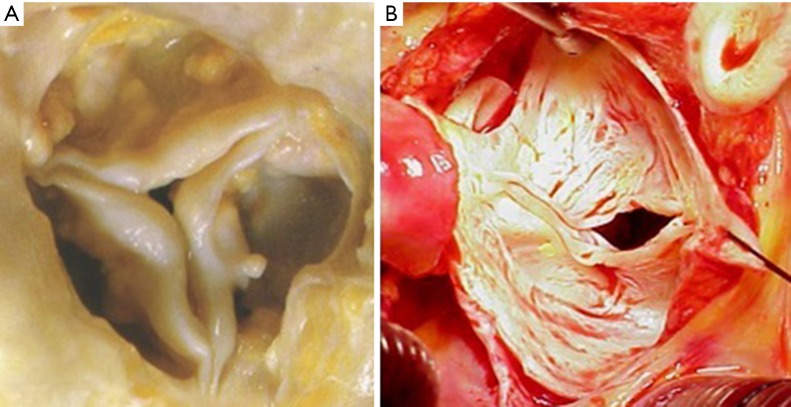
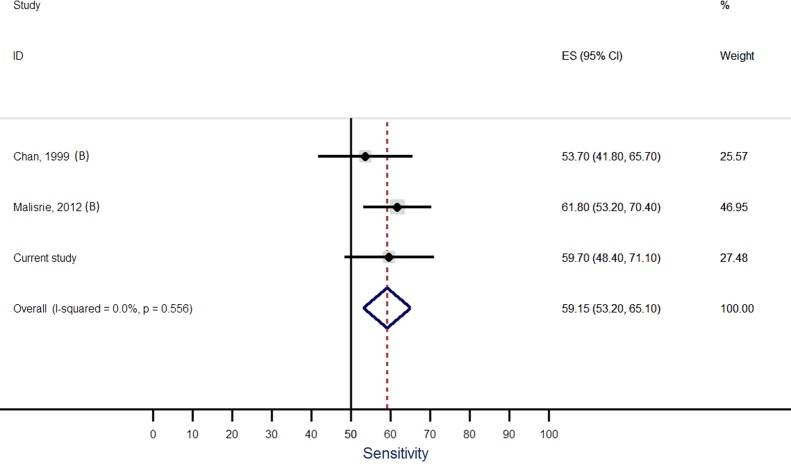
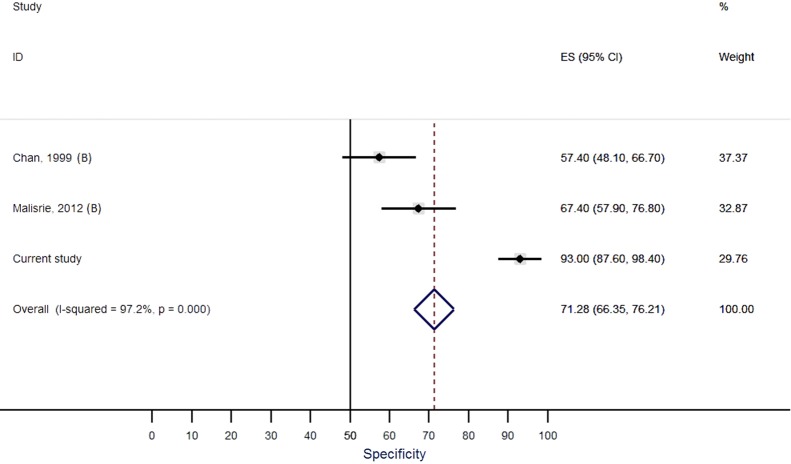
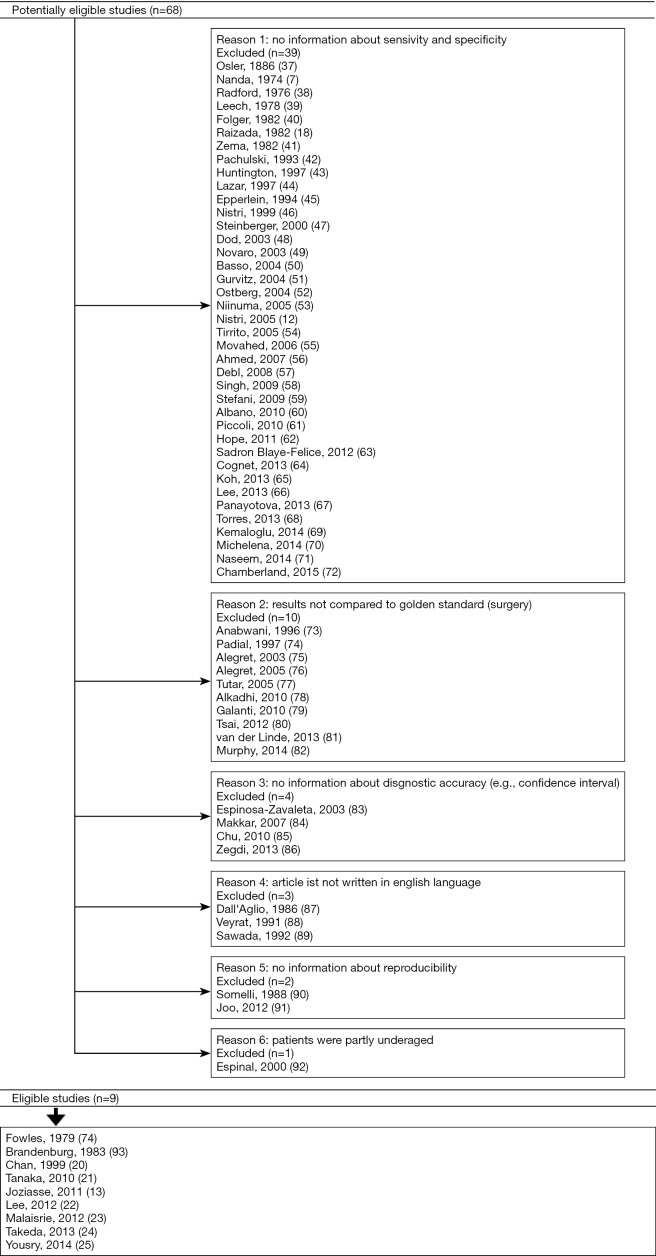
Methods: This retrospective, cross-sectional study of 216 adults included 132 men aged 62±14 years. Of these, 108 had BAV and 108 were age-matched individuals with TAV. All diagnoses were confirmed at surgery. We assessed TTE in two patient groups. First, in the (I) group of all 216 individuals, where we assessed accuracy for BAV according to the original diagnoses as documented by the primary investigators during original TTE examination. Second, we assessed accuracy for BAV according to expert re-evaluation in (II) all 158 TTE with availability of original recordings. Third, we performed a meta-analysis of published results on the accuracy of TTE for BAV according to PRISMA standards.
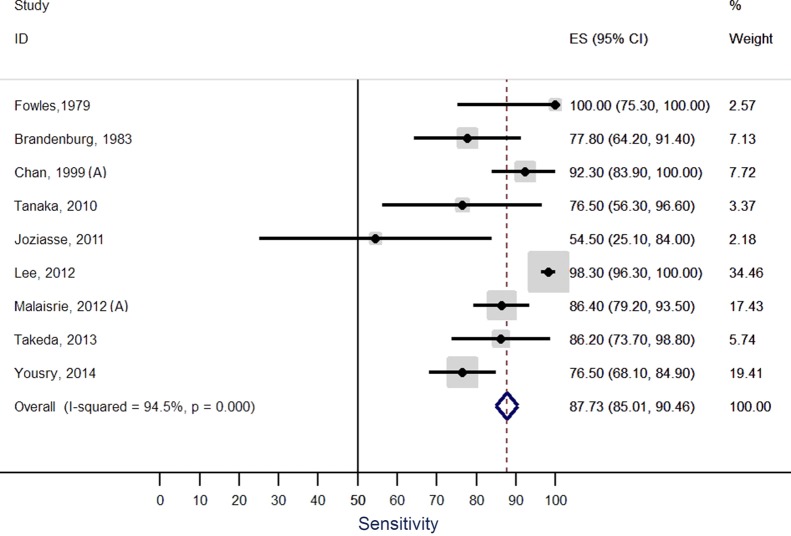
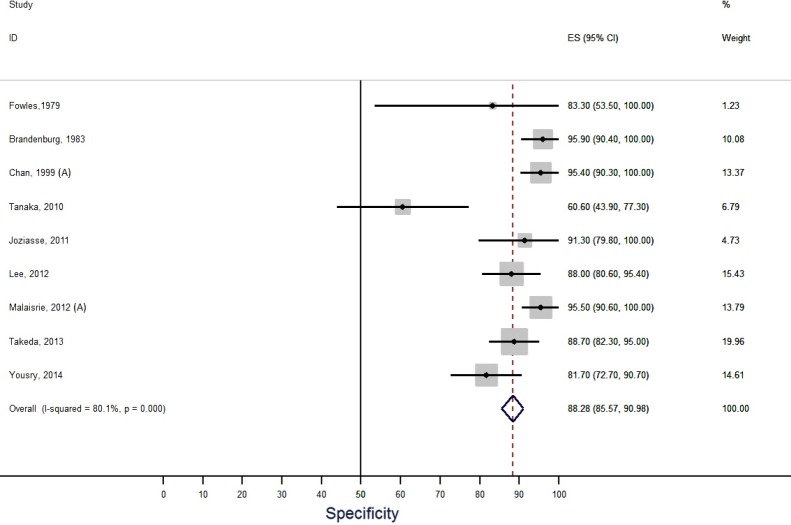
Results: Sensitivity, specificity and accuracy of (I) primary investigators was 46.3%, 97.2, and 71.8% as compared to (II) expert re-evaluation with 59.7%, 93%, and 77.8%, respectively. Sensitivity was significantly higher at re-evaluation (P<0.001). TTE at a non-tertiary care center (P=0.012), presence of aortic aneurysm (P=0.001) and presence of severe aortic valve calcification (P=0.003) predicted an inaccurate diagnosis of BAV. Conversely, meta-analysis of published TTE studies identified a pooled sensitivity of 87.7% and a pooled specificity of 88.3% for BAV.
Conclusions: The current study shows that TTE yields almost ideal diagnostic accuracy when ideal investigators examine ideal patients. However, the study also shows that TTE yields suboptimal diagnostic accuracy under routine conditions. TTE in non-tertiary care settings, concomitant aortic aneurysm, and presence of severe aortic valve calcification predict an inaccurate diagnosis of BAV.
Keywords: Bicuspid aortic valve (BAV); aorta; diagnostic error; echocardiography; evidence; meta-analysis.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- von Kodolitsch Y, Kaemmerer H. Bicuspid aortic valve. In: Niwa K, Kaemmerer H. editors. Aortopathy. Tokyo: Springer Japan, 2017:229-56.
LinkOut - more resources
Full Text Sources
Other Literature Sources