

The association of postoperative pulmonary complications in 109,360 patients with pressure-controlled or volume-controlled ventilation
- PMID: 28891046
- PMCID: PMC6696935
- DOI: 10.1111/anae.14039
The association of postoperative pulmonary complications in 109,360 patients with pressure-controlled or volume-controlled ventilation
Abstract
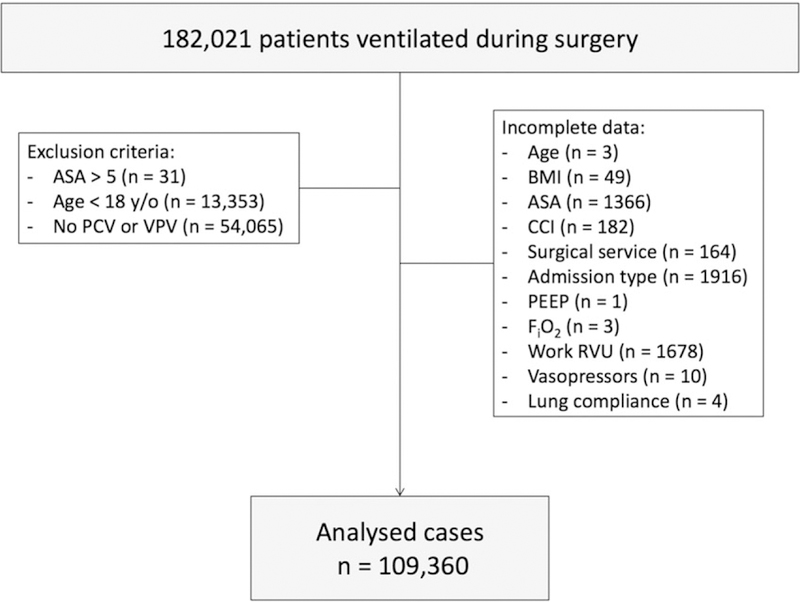
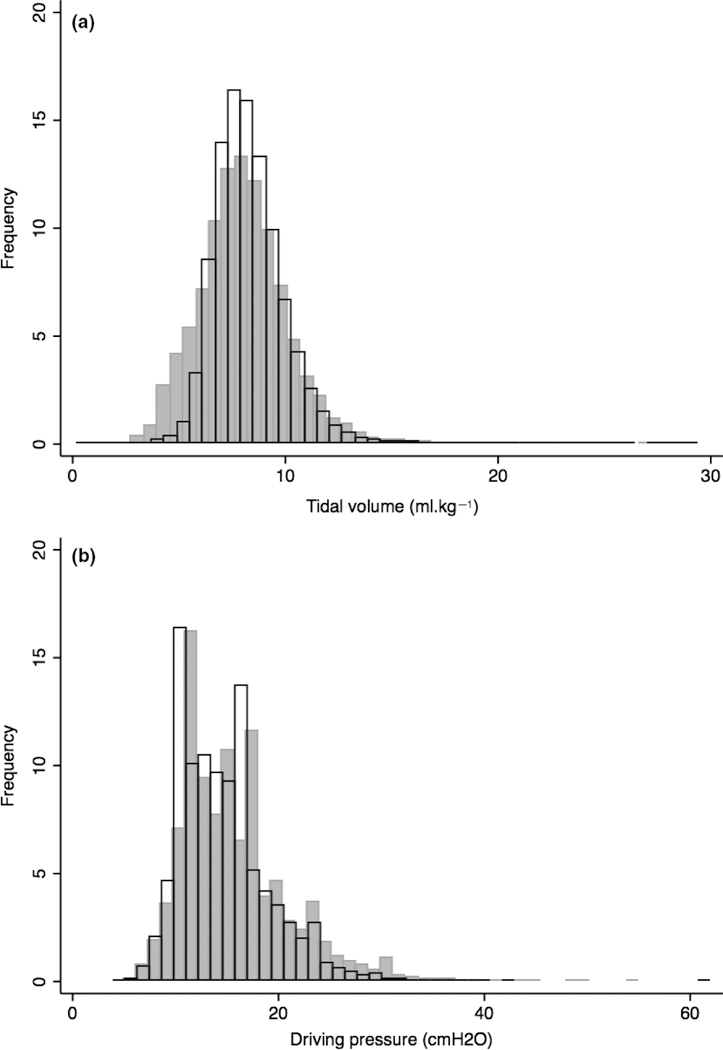
We thought that the rate of postoperative pulmonary complications might be higher after pressure-controlled ventilation than after volume-controlled ventilation. We analysed peri-operative data recorded for 109,360 adults, whose lungs were mechanically ventilated during surgery at three hospitals in Massachusetts, USA. We used multivariable regression and propensity score matching. Postoperative pulmonary complications were more common after pressure-controlled ventilation, odds ratio (95%CI) 1.29 (1.21-1.37), p < 0.001. Tidal volumes and driving pressures were more varied with pressure-controlled ventilation compared with volume-controlled ventilation: mean (SD) variance from the median 1.61 (1.36) ml.kg-1 vs. 1.23 (1.11) ml.kg-1 , p < 0.001; and 3.91 (3.47) cmH2 O vs. 3.40 (2.69) cmH2 O, p < 0.001. The odds ratio (95%CI) of pulmonary complications after pressure-controlled ventilation compared with volume-controlled ventilation at positive end-expiratory pressures < 5 cmH2 O was 1.40 (1.26-1.55) and 1.20 (1.11-1.31) when ≥ 5 cmH2 O, both p < 0.001, a relative risk ratio of 1.17 (1.03-1.33), p = 0.023. The odds ratio (95%CI) of pulmonary complications after pressure-controlled ventilation compared with volume-controlled ventilation at driving pressures of < 19 cmH2 O was 1.37 (1.27-1.48), p < 0.001, and 1.16 (1.04-1.30) when ≥ 19 cmH2 O, p = 0.011, a relative risk ratio of 1.18 (1.07-1.30), p = 0.016. Our data support volume-controlled ventilation during surgery, particularly for patients more likely to suffer postoperative pulmonary complications.
Keywords: lung protection ventilation: pressure goal; pressure-controlled ventilation; volume-controlled ventilation.
© 2017 The Association of Anaesthetists of Great Britain and Ireland.
Figures
 ) and volume-controlled ventilation (
) and volume-controlled ventilation ( ) during surgery in 18,268 patients and 91,092 patients, respectively.
) during surgery in 18,268 patients and 91,092 patients, respectively.Comment in
-
Mechanical ventilation mode and postoperative pulmonary complications.Anaesthesia. 2018 Feb;73(2):252-253. doi: 10.1111/anae.14195. Anaesthesia. 2018. PMID: 29333714 No abstract available.
-
Strategies for the prevention of postoperative pulmonary complications.Anaesthesia. 2018 Aug;73(8):923-927. doi: 10.1111/anae.14288. Epub 2018 Mar 26. Anaesthesia. 2018. PMID: 29582408 No abstract available.
-
Evidence for harms of high tidal volumes from systematic reviews and meta analysis.Anaesthesia. 2019 Aug;74(8):1070. doi: 10.1111/anae.14759. Anaesthesia. 2019. PMID: 31282576 No abstract available.
References
-
- Guay J, Ochroch EA. Intraoperative use of low volume ventilation to decrease postoperative mortality, mechanical ventilation, lengths of stay and lung injury in patients without acute lung injury. Cochrane Database of Systematic Reviews 2015; 12: CD011151. - PubMed
-
- Futier E, Constantin JM, Paugam-Burtz C, et al. A trial of intra-operative low-tidal-volume ventilation in abdominal surgery. New England Journal of Medicine 2013; 369: 428–37. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
