

Needle and syringe programmes and opioid substitution therapy for preventing HCV transmission among people who inject drugs: findings from a Cochrane Review and meta-analysis
- PMID: 28891267
- PMCID: PMC5836947
- DOI: 10.1111/add.14012
Needle and syringe programmes and opioid substitution therapy for preventing HCV transmission among people who inject drugs: findings from a Cochrane Review and meta-analysis
Abstract
Aims: To estimate the effects of needle and syringe programmes (NSP) and opioid substitution therapy (OST), alone or in combination, for preventing acquisition of hepatitis C virus (HCV) in people who inject drugs (PWID).
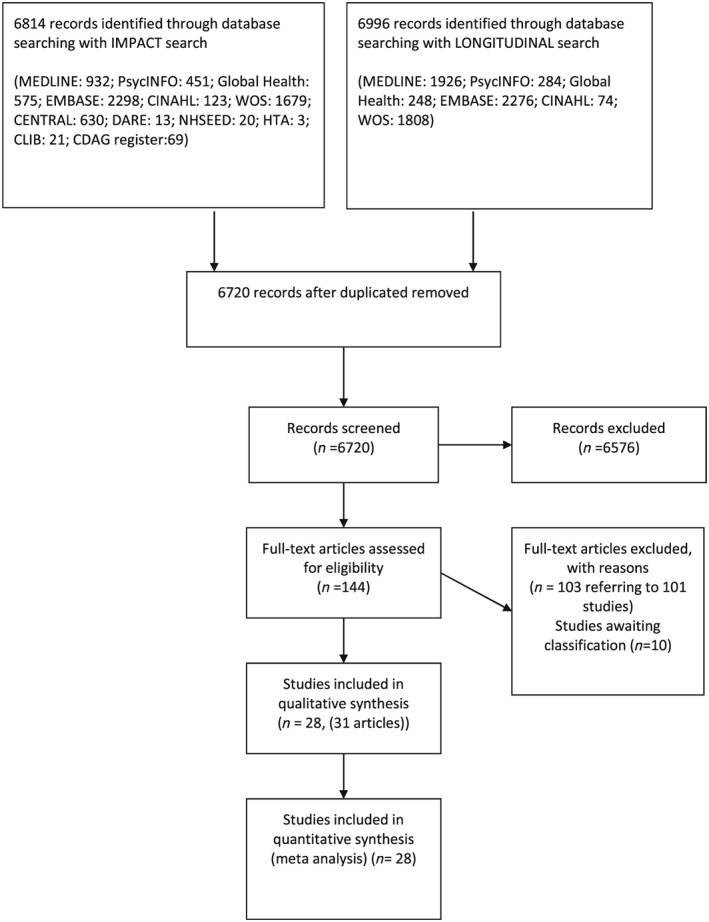
Methods: Systematic review and meta-analysis. Bibliographic databases were searched for studies measuring concurrent exposure to current OST (within the last 6 months) and/or NSP and HCV incidence among PWID. High NSP coverage was defined as regular NSP attendance or ≥ 100% coverage (receiving sufficient or greater number of needles and syringes per reported injecting frequency). Studies were assessed using the Cochrane risk of bias in non-randomized studies tool. Random-effects models were used in meta-analysis.
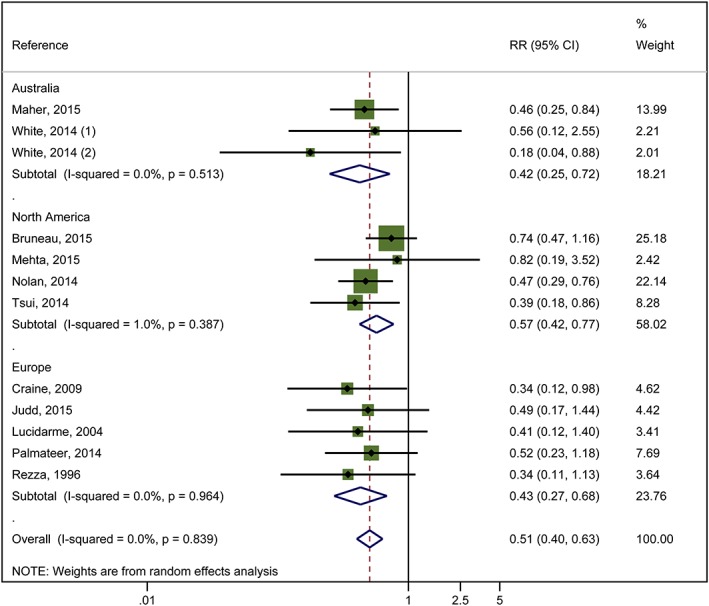
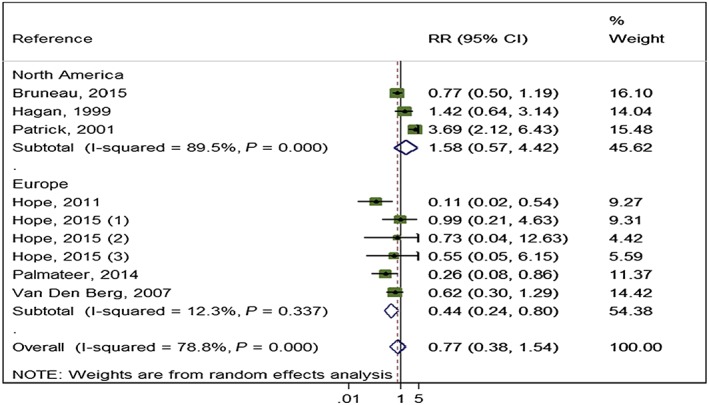
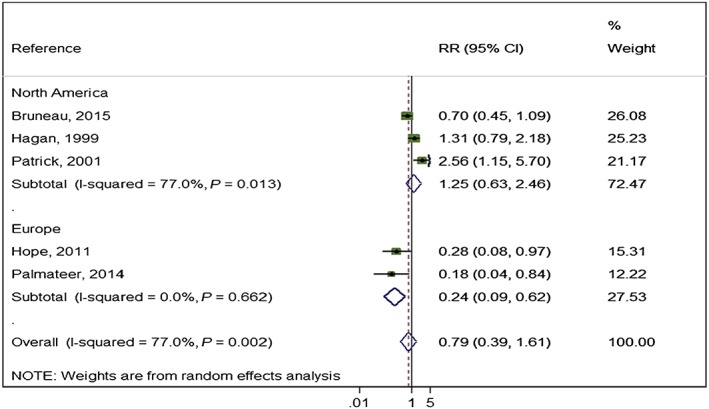
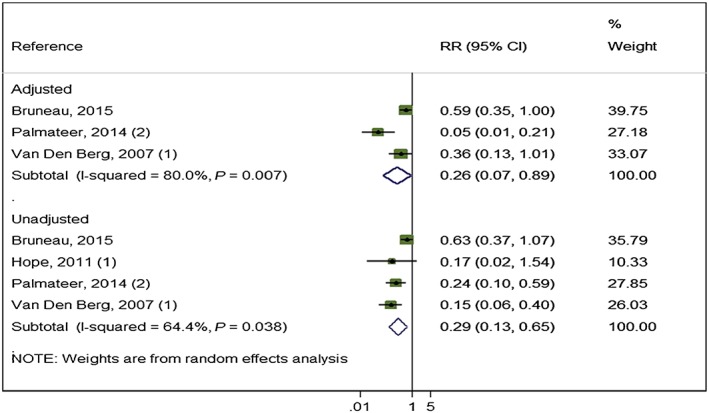
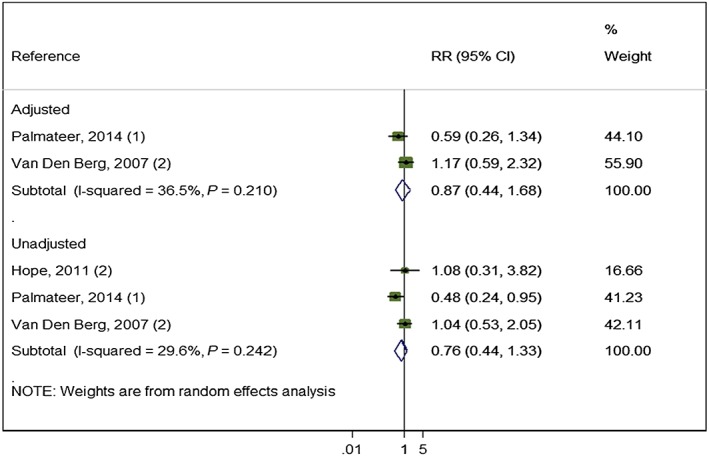
Results: We identified 28 studies (n = 6279) in North America (13), United Kingdom (five), Europe (four), Australia (five) and China (one). Studies were at moderate (two), serious (17) critical (seven) and non-assessable risk of bias (two). Current OST is associated with 50% [risk ratio (RR) =0.50, 95% confidence interval (CI) = 0.40-0.63] reduction in HCV acquisition risk, consistent across region and with low heterogeneity (I2 = 0, P = 0.889). Weaker evidence was found for high NSP coverage (RR = 0.79, 95% CI = 0.39-1.61) with high heterogeneity (I2 = 77%, P = 0.002). After stratifying by region, high NSP coverage in Europe was associated with a 56% reduction in HCV acquisition risk (RR = 0.44, 95% CI = 0.24-0.80) with low heterogeneity (I2 = 12.3%, P = 0.337), but not in North America (RR = 1.58, I2 = 89.5%, P = < 0.001). Combined OST/NSP is associated with a 74% reduction in HCV acquisition risk (RR = 0.26, 95% CI = 0.07-0.89, I2 = 80% P = 0.007). According to Grades of Recommendation Assessment, Development and Evaluation (GRADE) criteria, the evidence on OST and combined OST/NSP is low quality, while NSP is very low.
Conclusions: Opioid substitution therapy reduces risk of hepatitis C acquisition and is strengthened in combination with needle and syringe programmes (NSP). There is weaker evidence for the impact of needle syringe programmes alone, although stronger evidence that high coverage is associated with reduced risk in Europe.
Keywords: Cochrane; harm reduction; hepatitis C; incidence; meta-analysis; needle and syringe programmes; opioid substitution therapy; review; substance use.
© 2017 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures
References
-
- Gower E., Estes C., Blach S., Razavi‐Shearer K., Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014; 61: S45–S57. - PubMed
-
- Mohd Hanafiah K., Groeger J., Flaxman A. D., Wiersma S. T. Global epidemiology of hepatitis C virus infection: new estimates of age‐specific antibody to HCV seroprevalence. Hepatol (Balt) 2013; 57: 1333–1342. - PubMed
-
- Perz J. F., Armstrong G. L., Farrington L. A., Hutin Y. J., Bell B. P. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol 2006; 45: 529–538. - PubMed
-
- Degenhardt L., Charlson F., Stanaway J., Larney S., Alexander L. T., Hickman M. et al Estimating the burden of disease attributable to injecting drug use as a risk factor for HIV, hepatitis C, and hepatitis B: findings from the global burden of disease study. Lancet Infect Dis 2013; 16: 1385–1398. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
