

Towards Chagas disease elimination: Neonatal screening for congenital transmission in rural communities
- PMID: 28892479
- PMCID: PMC5634652
- DOI: 10.1371/journal.pntd.0005783
Towards Chagas disease elimination: Neonatal screening for congenital transmission in rural communities
Abstract
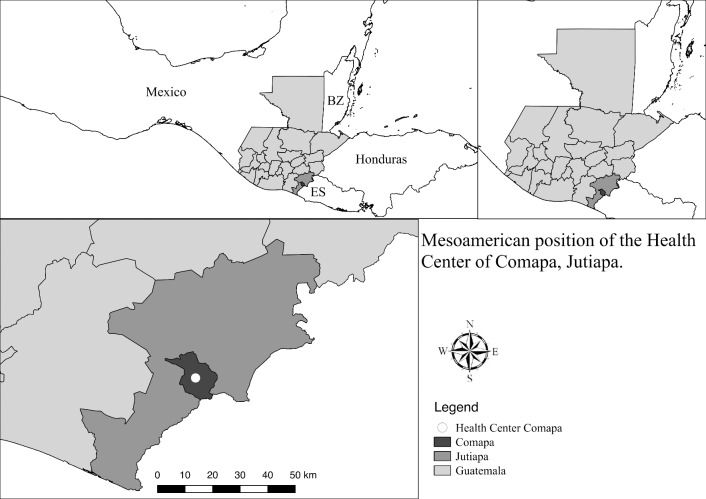
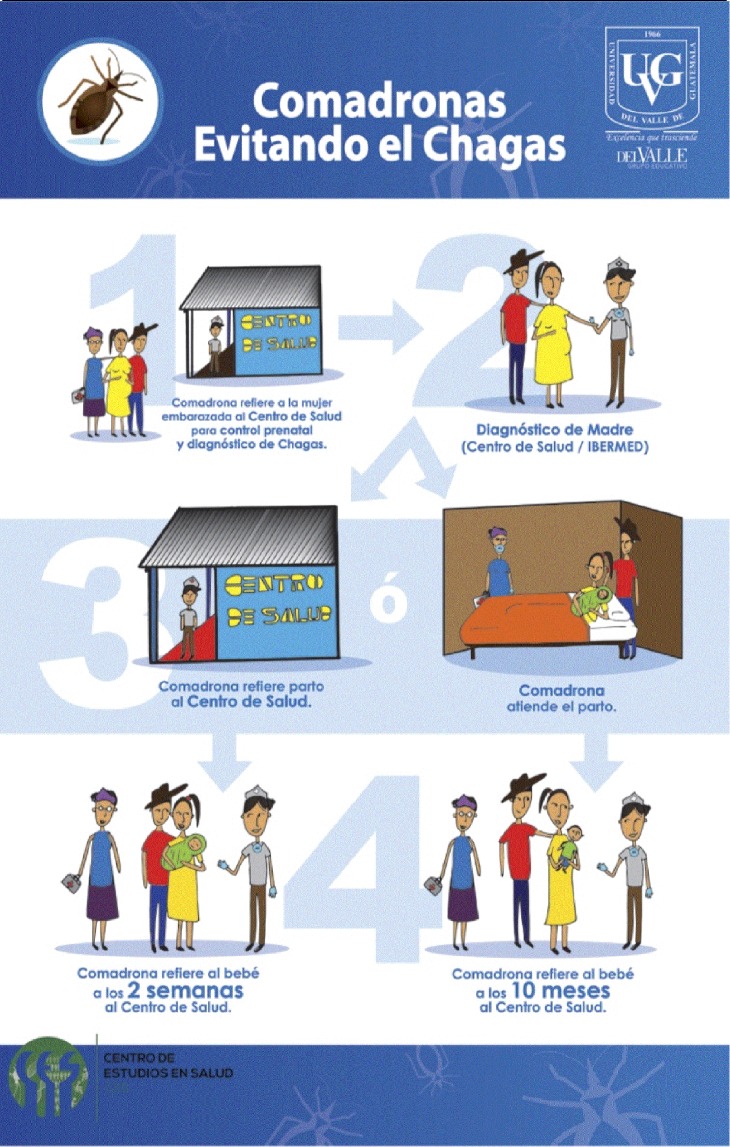
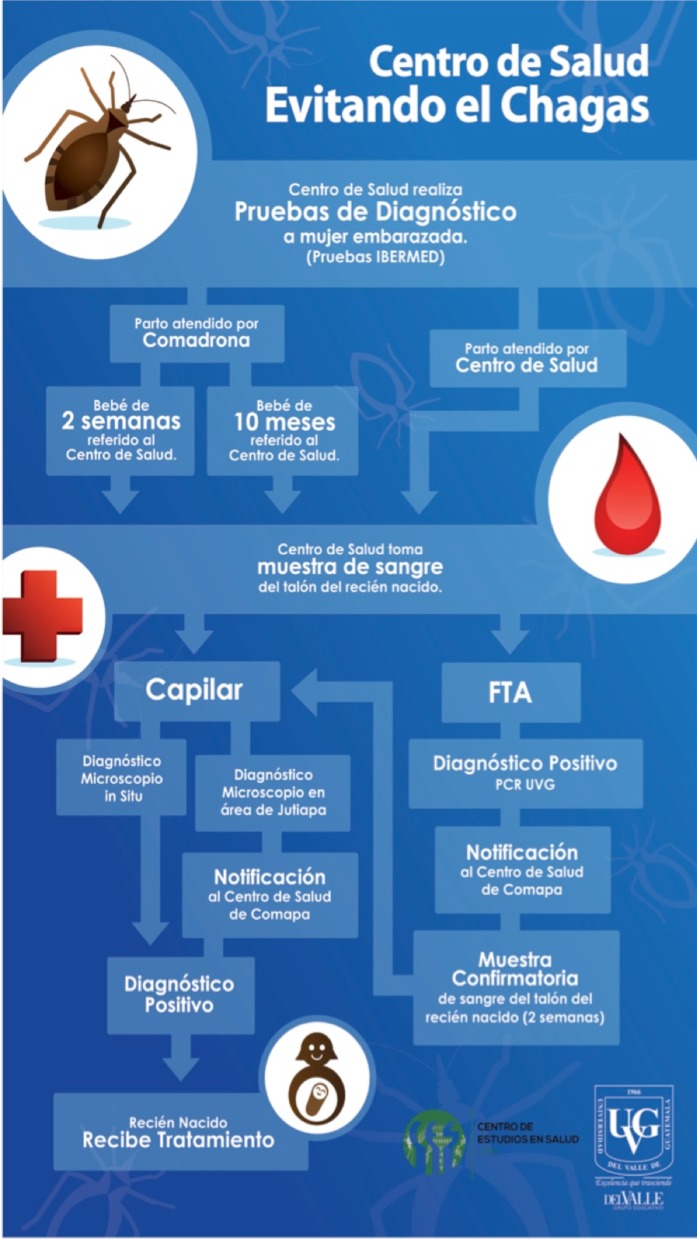
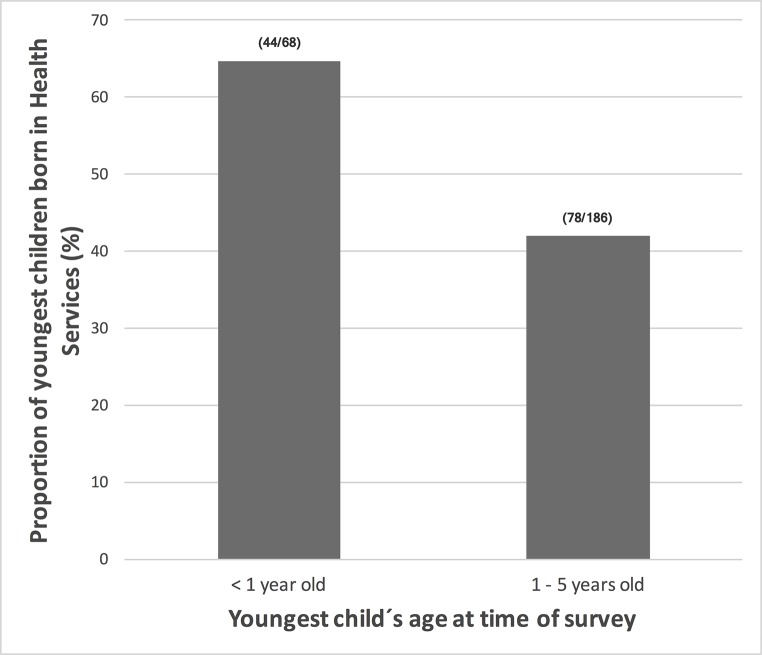
Chagas disease is a neglected tropical disease that continues to affect populations living in extreme poverty in Latin America. After successful vector control programs, congenital transmission remains as a challenge to disease elimination. We used the PRECEDE-PROCEED planning model to develop strategies for neonatal screening of congenital Chagas disease in rural communities of Guatemala. These communities have persistent high triatomine infestations and low access to healthcare. We used mixed methods with multiple stakeholders to identify and address maternal-infant health behaviors through semi-structured interviews, participatory group meetings, archival reviews and a cross-sectional survey in high risk communities. From December 2015 to April 2016, we jointly developed a strategy to illustratively advertise newborn screening at the Health Center. The strategy included socioculturally appropriate promotional and educational material, in collaboration with midwives, nurses and nongovernmental organizations. By March 2016, eight of 228 (3.9%) pregnant women had been diagnosed with T. cruzi at the Health Center. Up to this date, no neonatal screening had been performed. By August 2016, seven of eight newborns born to Chagas seropositive women had been parasitologically screened at the Health Center, according to international standards. Thus, we implemented a successful community-based neonatal screening strategy to promote congenital Chagas disease healthcare in a rural setting. The success of the health promotion strategies developed will depend on local access to maternal-infant services, integration with detection of other congenital diseases and reliance on community participation in problem and solution definition.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hashimoto K, Alvarez H, Nakagawa J, Juarez J, Monroy C, Cordón-Rosales C, Gil E. Vector control intervention towards interruption of transmission of Chagas disease by Rhodnius prolixus, main vector in Guatemala. Mem. Inst. Oswaldo Cruz 2012; 107: 877–887. - PubMed
-
- Ministerio de Salud de la Nación. Enfermedades infecciosas Chagas, atención del paciente con enfermedad de Chagas. Minist. Salud Argentina 2010; 7: 1–35.Available from: http://www.msal.gob.ar/images/stories/epidemiologia/pdf/guia-medica-equi...
-
- Rendell VR, Gilman RH, Galdos-Cardenas G, Valencia E, Verastegui M, Sanchez L, et al. Trypanosoma cruzi-infected pregnant women without vector exposure have higher parasitemia levels: implications for congenital transmission risk. PLoS One 2015; 10: p. e0119527 doi: 10.1371/journal.pone.0119527 - DOI - PMC - PubMed
-
- Brutus L, Castillo H, Bernal C, Salas NA, Schneider D, Santalla JA, et al. Short report: Detectable Trypanosoma cruzi parasitemia during pregnancy and delivery as a risk factor for congenital chagas disease. Am. J. Trop. Med. Hyg. 2010; 83: 1044–1047. doi: 10.4269/ajtmh.2010.10-0326 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
