

Accuracy of Complete Blood Cell Counts to Identify Febrile Infants 60 Days or Younger With Invasive Bacterial Infections
- PMID: 28892537
- PMCID: PMC6583058
- DOI: 10.1001/jamapediatrics.2017.2927
Accuracy of Complete Blood Cell Counts to Identify Febrile Infants 60 Days or Younger With Invasive Bacterial Infections
Erratum in
-
Error in Key Points.JAMA Pediatr. 2018 Mar 1;172(3):302. doi: 10.1001/jamapediatrics.2017.5387. JAMA Pediatr. 2018. PMID: 29309481 Free PMC article. No abstract available.
Abstract
Importance: Clinicians often risk stratify young febrile infants for invasive bacterial infections (IBIs), defined as bacteremia and/or bacterial meningitis, using complete blood cell count parameters.
Objective: To estimate the accuracy of individual complete blood cell count parameters to identify febrile infants with IBIs.
Design, setting, and participants: Planned secondary analysis of a prospective observational cohort study comprising 26 emergency departments in the Pediatric Emergency Care Applied Research Network from 2008 to 2013. We included febrile (≥38°C), previously healthy, full-term infants younger than 60 days for whom blood cultures were obtained. All infants had either cerebrospinal fluid cultures or 7-day follow-up.
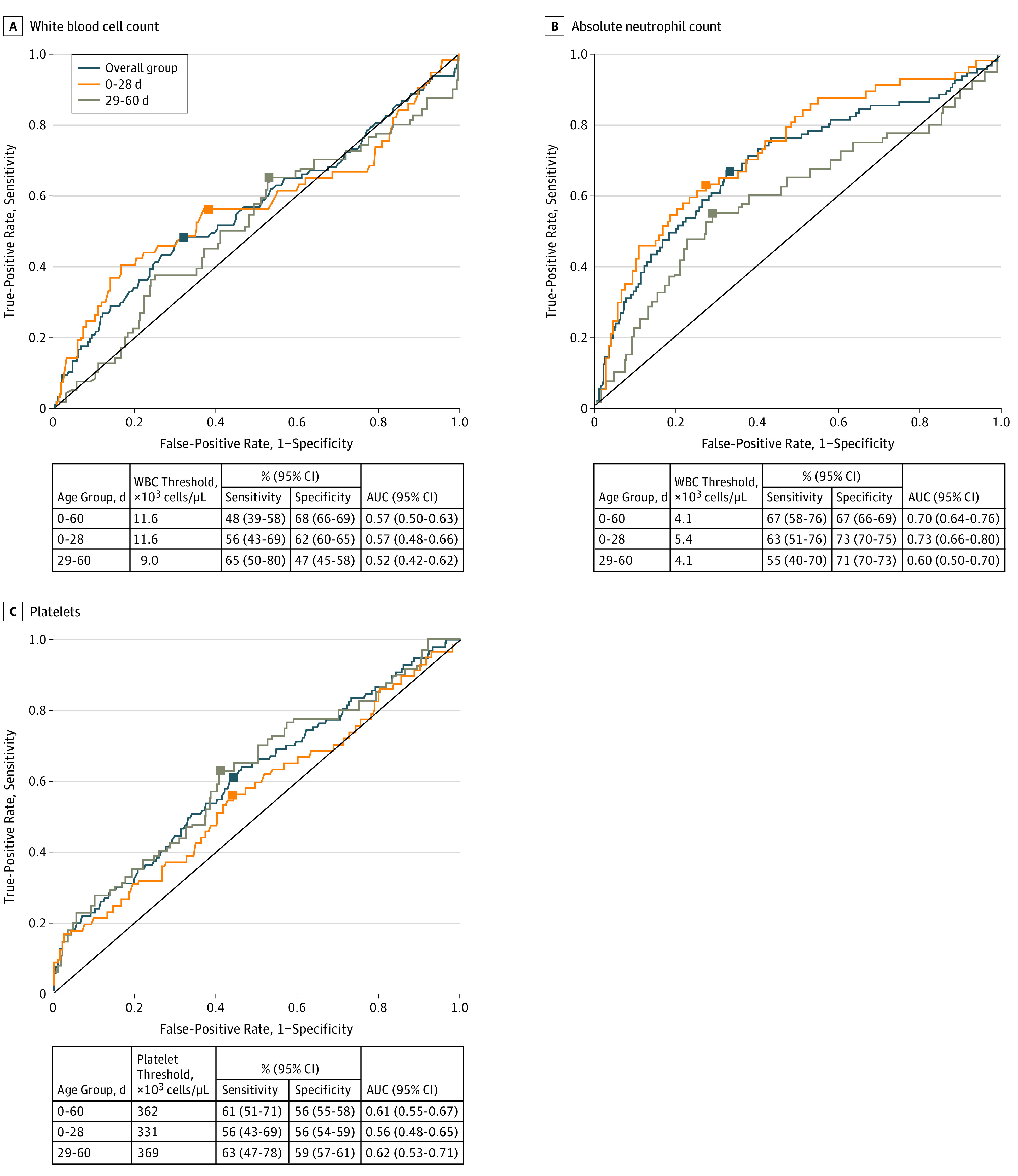
Main outcomes and measures: We tested the accuracy of the white blood cell count, absolute neutrophil count, and platelet count at commonly used thresholds for IBIs. We determined optimal thresholds using receiver operating characteristic curves.
Results: Of 4313 enrolled infants, 1340 (31%; 95% CI, 30% to 32%) were aged 0 to 28 days, 2412 were boys (56%), and 2471 were white (57%). Ninety-seven (2.2%; 95% CI, 1.8% to 2.7%) had IBIs. Sensitivities were low for common complete blood cell count parameter thresholds: white blood cell count less than 5000/µL, 10% (95% CI, 4% to 16%) (to convert to 109 per liter, multiply by 0.001); white blood cell count ≥15 000/µL, 27% (95% CI, 18% to 36%); absolute neutrophil count ≥10 000/µL, 18% (95% CI, 10% to 25%) (to convert to × 109 per liter, multiply by 0.001); and platelets <100 × 103/µL, 7% (95% CI, 2% to 12%) (to convert to × 109 per liter, multiply by 1). Optimal thresholds for white blood cell count (11 600/µL), absolute neutrophil count (4100/µL), and platelet count (362 × 103/µL) were identified in models that had areas under the receiver operating characteristic curves of 0.57 (95% CI, 0.50-0.63), 0.70 (95% CI, 0.64-0.76), and 0.61 (95% CI, 0.55-0.67), respectively.
Conclusions and relevance: No complete blood cell count parameter at commonly used or optimal thresholds identified febrile infants 60 days or younger with IBIs with high accuracy. Better diagnostic tools are needed to risk stratify young febrile infants for IBIs.
Conflict of interest statement
Figures
References
-
- Gorelick MH, Alpern ER, Alessandrini EA. A system for grouping presenting complaints: the pediatric emergency reason for visit clusters. Acad Emerg Med. 2005;12(8):723-731. - PubMed
-
- Gomez B, Mintegi S, Bressan S, Da Dalt L, Gervaix A, Lacroix L; European Group for Validation of the Step-by-Step Approach . Validation of the “Step-by-Step” approach in the management of young febrile infants. Pediatrics. 2016;138(2):e20154381. - PubMed
-
- Schnadower D, Kuppermann N, Macias CG, et al. ; American Academy of Pediatrics Pediatric Emergency Medicine Collaborative Research Committee . Febrile infants with urinary tract infections at very low risk for adverse events and bacteremia. Pediatrics. 2010;126(6):1074-1083. - PubMed
-
- Shah AP, Cobb BT, Lower DR, et al. Enhanced versus automated urinalysis for screening of urinary tract infections in children in the emergency department. Pediatr Infect Dis J. 2014;33(3):272-275. - PubMed
-
- Schroeder AR, Chang PW, Shen MW, Biondi EA, Greenhow TL. Diagnostic accuracy of the urinalysis for urinary tract infection in infants <3 months of age. Pediatrics. 2015;135(6):965-971. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
