

Association between carotid plaque characteristics and acute cerebral infarction determined by MRI in patients with type 2 diabetes mellitus
- PMID: 28893252
- PMCID: PMC5594451
- DOI: 10.1186/s12933-017-0592-9
Association between carotid plaque characteristics and acute cerebral infarction determined by MRI in patients with type 2 diabetes mellitus
Abstract
Background: Type 2 diabetes mellitus (T2DM) might aggravate the carotid plaque vulnerability, and increase the risk for ischemic stroke. Few studies reported the acute stroke subtype with carotid plaque characteristics in T2DM patients. This study aimed to investigate the association between carotid plaque characteristics and acute cerebral infarct (ACI) lesion features determined by MRI in T2DM patients.
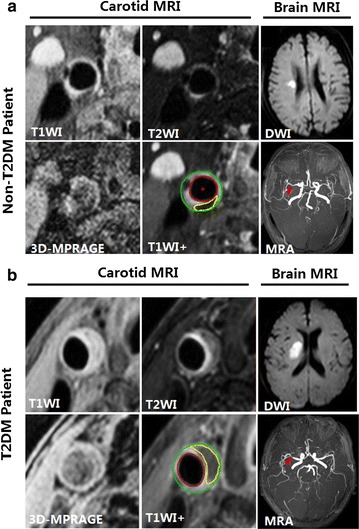
Methods: Patients with acute cerebrovascular syndrome in internal carotid artery territory were recruited. All patients were stratified into T2DM and non-T2DM groups and underwent both carotid and brain MRI scans. Ipsilateral carotid plaque morphological and compositional characteristics, intracranial and extracranial carotid artery stenosis were also determined. Stroke subtype based on the Trial of ORG 10172 in Acute Stroke Treatment classification and ACI lesion patterns were evaluated.
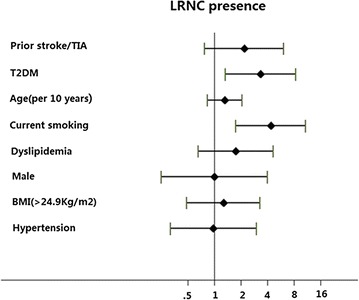
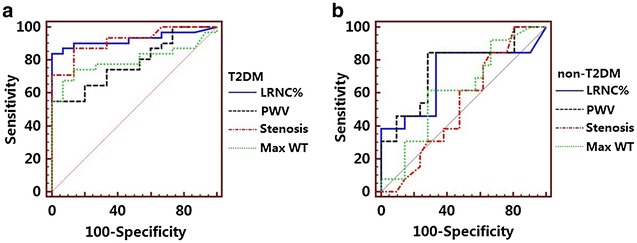
Results: Of the recruited 140 patients, 68 (48.6%) patients had T2DM (mean age 64.16 ± 11.38 years, 40 males). T2DM patients exhibited higher prevalence of carotid type IV-VI lesions, larger plaque burden as well as larger lipid-rich necrotic core (LRNC) compared with non-T2DM patients. Among the patients with carotid LRNC on symptomatic side, more concomitant large perforating artery infarct patterns and larger ACI size in the internal carotid artery territory were found in T2DM group than those in non-T2DM group. Carotid plaque with LRNC% > 22.0% was identified as an independent risk factor for the presence of ACI lesions confined to the carotid territory in T2DM patients, regardless of other risk factors.
Conclusions: This study shows that more concomitant large perforating artery infarct patterns and larger ACI size in the internal carotid artery territory were found in the T2DM patients with ipsilateral carotid LRNC plaque than those in non-T2DM patients. Quantification of the carotid plaque characteristics, particularly the LRNC% by MRI has the potential usefulness for stroke risk stratification.
Keywords: Acute stroke; Carotid plaque; Diabetes mellitus; Lipid-rich necrotic core; MR imaging.
Figures
References
-
- Ibebuogu UN, Nasir K, Gopal A, Ahmadi N, Mao SS, Young E, Honoris L, Nuguri VK, Lee RS, Usman N, et al. Comparison of atherosclerotic plaque burden and composition between diabetic and non diabetic patients by non invasive CT angiography. Int J Cardiovasc Imaging. 2009;25(7):717–723. doi: 10.1007/s10554-009-9483-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
