

Antiretroviral therapy for pregnant women living with HIV or hepatitis B: a systematic review and meta-analysis
- PMID: 28893758
- PMCID: PMC6027063
- DOI: 10.1136/bmjopen-2017-019022
Antiretroviral therapy for pregnant women living with HIV or hepatitis B: a systematic review and meta-analysis
Abstract
Objective: To assess the impact of various antiretroviral/antiviral regimens in pregnant women living with HIV or hepatitis B virus (HBV).
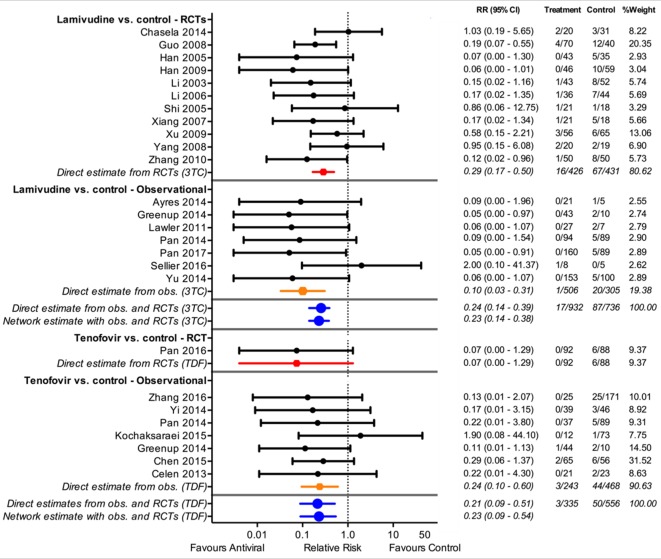
Design: We performed random effects meta-analysis for HIV-related outcomes and network meta-analysis for HBV outcomes, and used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to assess quality separately for each outcome.
Data sources: Embase and Medline to February 2017.
Eligibility criteria: For maternal outcomes, we considered randomised controlled trials (RCTs) comparing tenofovir-based regimens with those with alternative nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs). For child outcomes, we included RCTs and comparative observational studies of tenofovir-based regimens versus alternative NRTIs regimens or, for HBV, placebo.
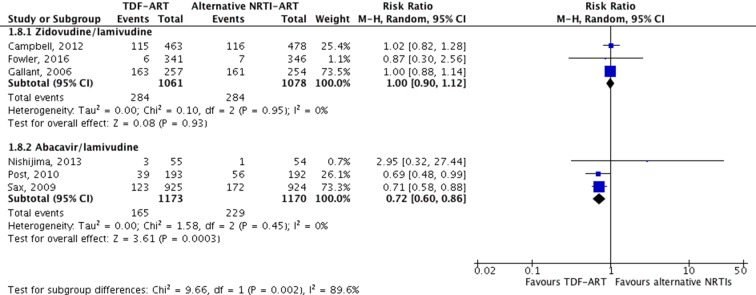
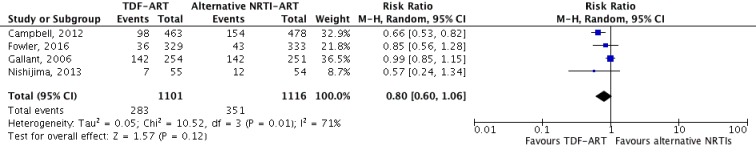
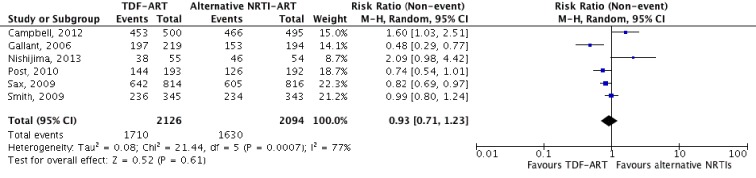
Results: Ten studies (seven RCTs) met the inclusion criteria for maternal and child outcomes, and an additional 33 studies (12 RCTs) met the inclusion criteria for HBV-specific outcomes. The most common comparison was tenofovir and emtricitabine versus zidovudine and lamivudine. There was no apparent difference between tenofovir-based regimens and alternatives in maternal outcomes, including serious laboratory adverse events (low certainty) and serious clinical adverse events (moderate certainty). There was no difference between NRTIs in vertical transmission of HIV: 1 more per 1000, 8 fewer to 10 more, low certainty; or vertical transmission of HBV: 7 fewer per 1000, 10 fewer to 38 more, moderate certainty. We found moderate certainty evidence that tenofovir/emtricitabine increases the risk of stillbirths and early neonatal mortality (51 more per 1000, 11 more to 150 more) and the risk of early premature delivery at <34 weeks (42 more per 1000, 2 more to 127 more).
Conclusions: Tenofovir/emtricitabine is likely to increase stillbirth/early neonatal death and early premature delivery compared with zidovudine/lamivudine, but certainty is low when they are not coprescribed with lopinavir/ritonavir. Other outcomes are likely similar between antiretrovirals.
Trial registration number: PROSPERO CRD42017054392.
Keywords: HIV & AIDS; chronic hepatitis B; mother-to-child transmission; network meta-analysis; pregnancy; tenofovir.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: RAS, AM, YZ, and GHG are members of the GRADE Working Group. There are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- World Health Organization. Number of women living with HIV. Geneva, Switzerland: World Health Organization, 2017. http://www.who.int/gho/hiv/epidemic_status/cases_adults_women_children/en/ (accessed 20 Mar 2017).
-
- Rates of mother-to-child transmission of HIV-1 in Africa, America, and Europe: results from 13 perinatal studies. The Working Group on Mother-To-Child Transmission of HIV. J Acquir Immune Defic Syndr Hum Retrovirol 1995;8:506–10. - PubMed
-
- De Cock KM, Fowler MG, Mercier E, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA 2000;283:1175–82. - PubMed
-
- UNAIDS. HIV Fact Sheets, 2017. http://aidsinfo.unaids.org/ (accessed 20 Mar 2017).
-
- World Health Organization. Prevention of mother-to-child transmission: World Health Organization, 2017. Available from http://www.who.int/gho/hiv/epidemic_response/PMTCT_text/en/ (accessed 04 Nov 2017).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous