

Physician Support of Smoking Cessation After Diagnosis of Lung, Bladder, or Upper Aerodigestive Tract Cancer
- PMID: 28893814
- PMCID: PMC5593727
- DOI: 10.1370/afm.2100
Physician Support of Smoking Cessation After Diagnosis of Lung, Bladder, or Upper Aerodigestive Tract Cancer
Abstract
Purpose: Smoking cessation after a diagnosis of lung, bladder, and upper aerodigestive tract cancer appears to improve survival, and support to quit would improve cessation. The aims of this study were to assess how often general practitioners provide active smoking cessation support for these patients and whether physician behavior is influenced by incentive payments.
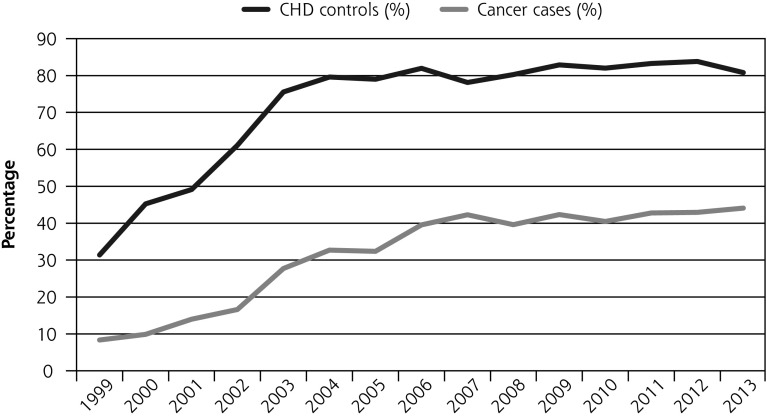
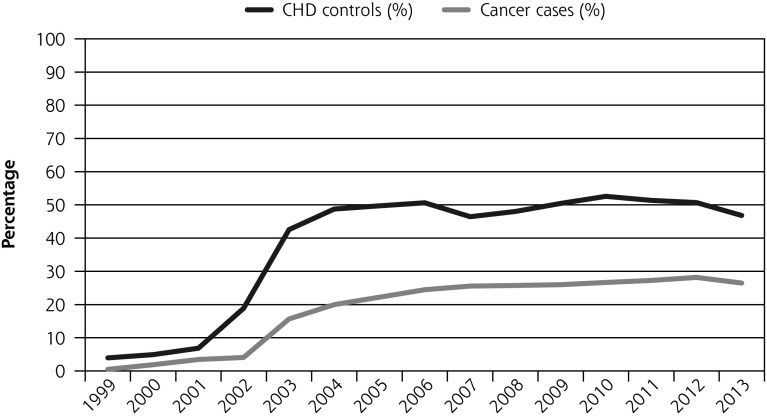
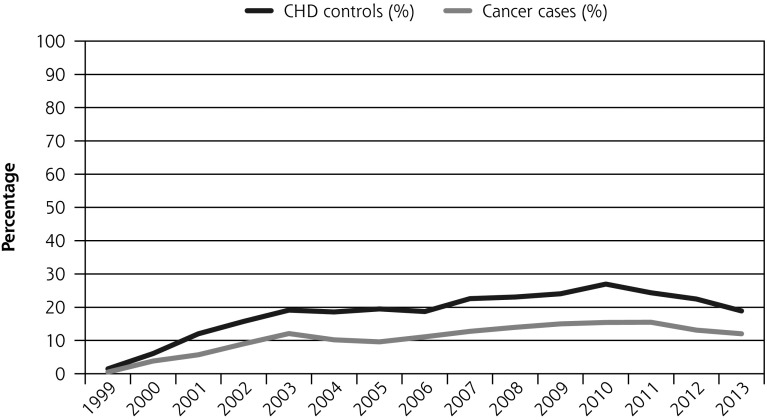
Methods: Using electronic primary care records from the UK Clinical Practice Research Datalink, 12,393 patients with incident cases of cancer diagnosed between 1999 and 2013 were matched 1 to 1 to patients with incident cases of coronary heart disease (CHD) diagnosed during the same time. We assessed differences in the proportion for whom physicians updated smoking status, advised quitting, and prescribed cessation medications, as well as the proportion of patients who stopped smoking within a year of diagnosis. We further examined whether any differences arose because the physicians were offered incentives to address smoking in patients with CHD and not cancer.
Results: At diagnosis, 32.0% of patients with cancer and 18.2% of patients with CHD smoked tobacco. Patients with cancer were less likely than patients with CHD to have their general practitioners update smoking status (OR = 0.18; 95% CI, 0.17-0.19), advise quitting (OR = 0.38; 95% CI, 0.36-0.40), or prescribe medication (OR = 0.67; 95% CI, 0.63-0.73), and they were less likely to have stopped smoking (OR = 0.76; 95% CI, 0.69-0.84). One year later 61.7% of patients with cancer and 55.4% with CHD who were smoking at diagnosis were still smoking. Introducing incentive payments was associated with more frequent interventions, but not for patients with CHD specifically.
Conclusions: General practitioners were less likely to support smoking cessation in patients with cancer than with CHD, and patients with cancer were less likely to stop smoking. This finding is not due to the difference in incentive payments.
Keywords: cancer; primary care; smoking; smoking cessation.
© 2017 Annals of Family Medicine, Inc.
Conflict of interest statement
Conflicts of interest: P.A. reports grants from the Medical Research Council (MRC), National Institute for Health Research (NIHR), Cancer Research UK (CRUK), Economic and Social Research Council, and UK Centre for Tobacco and Alcohol Studies during the conduct of this study; A.F. reports grants from the NIHR, MRC, and CRUK during the conduct of this study; R.R. reports that he was partly funded by the National Health Service (NHS) (Heart of England NHS Foundation Trust) during the conduct of this study. All other authors report none.
Figures
References
-
- Cancer Research UK. CRUK 2015 Cancer incidence for common cancers. 2015. http://www.cancerresearchuk.org/health-professional/cancer-statistics/in....
-
- US Surgeon General. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Washington, DC: US Department of Health and Human Services; 2014.
-
- Aveyard P, Adab P, Cheng KK, Wallace DM, Hey K, Murphy MF. Does smoking status influence the prognosis of bladder cancer? A systematic review. BJU Int. 2002;90(3):228–239. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical