

The MUC5B promoter polymorphism is associated with specific interstitial lung abnormality subtypes
- PMID: 28893869
- PMCID: PMC5687883
- DOI: 10.1183/13993003.00537-2017
The MUC5B promoter polymorphism is associated with specific interstitial lung abnormality subtypes
Abstract
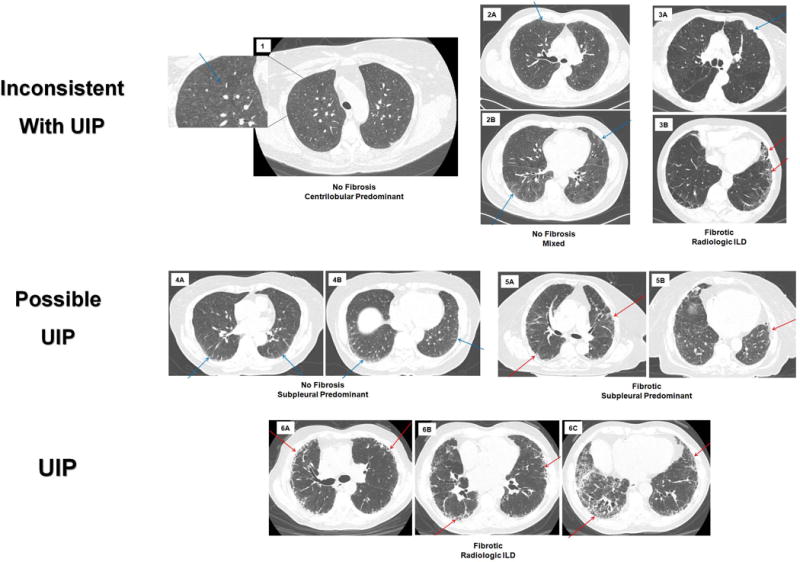
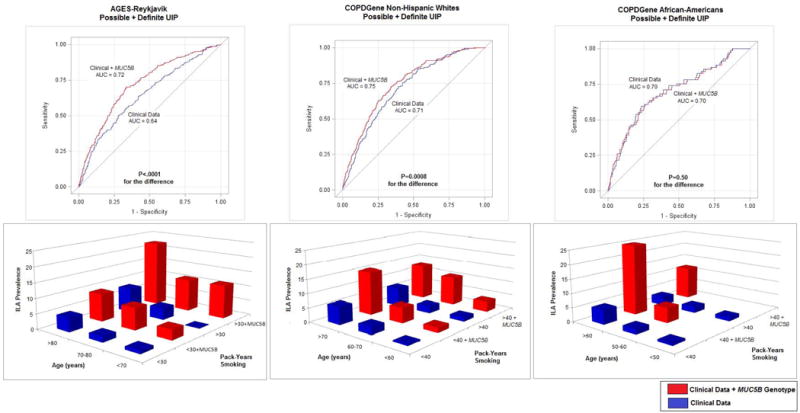
The MUC5B promoter polymorphism (rs35705950) has been associated with interstitial lung abnormalities (ILA) in white participants from the general population; whether these findings are replicated and influenced by the ILA subtype is not known. We evaluated the associations between the MUC5B genotype and ILA in cohorts with extensive imaging characterisation.We performed ILA phenotyping and MUC5B promoter genotyping in 5308 and 9292 participants from the AGES-Reykjavik and COPDGene cohorts, respectively.We found that ILA was present in 7% of participants from the AGES-Reykjavik, 8% of non-Hispanic white participants from COPDGene and 7% of African-American participants from COPDGene. Although the MUC5B genotype was strongly associated (after correction for multiple testing) with ILA (OR 2.1, 95% CI 1.8-2.4, p=1×10-26), there was evidence of significant heterogeneity between cohorts (I2=81%). When narrowed to specific radiologic subtypes, (e.g. subpleural ILA), the MUC5B genotype remained strongly associated (OR 2.6, 95% CI 2.2-3.1, p=1×10-30) with minimal heterogeneity (I2=0%). Although there was no evidence that the MUC5B genotype influenced survival, there was evidence that MUC5B genotype improved risk prediction for possible usual interstitial pneumonia (UIP) or a UIP pattern in non-Hispanic white populations.The MUC5B promoter polymorphism is strongly associated with ILA and specific radiologic subtypes of ILA, with varying degrees of heterogeneity in the underlying populations.
The content of this work is not subject to copyright. Design and branding are copyright ©ERS 2017.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
Figures
References
-
- Washko GR, Hunninghake GM, Fernandez IE, Nishino M, Okajima Y, Yamashiro T, Ross JC, Estepar RS, Lynch DA, Brehm JM, Andriole KP, Diaz AA, Khorasani R, D’Aco K, Sciurba FC, Silverman EK, Hatabu H, Rosas IO, Investigators CO Lung volumes and emphysema in smokers with interstitial lung abnormalities. The New England journal of medicine. 2011;364(10):897–906. - PMC - PubMed
-
- Hunninghake GM, Hatabu H, Okajima Y, Gao W, Dupuis J, Latourelle JC, Nishino M, Araki T, Zazueta OE, Kurugol S, Ross JC, San Jose Estepar R, Murphy E, Steele MP, Loyd JE, Schwarz MI, Fingerlin TE, Rosas IO, Washko GR, O’Connor GT, Schwartz DA. MUC5B promoter polymorphism and interstitial lung abnormalities. The New England journal of medicine. 2013;368(23):2192–2200. - PMC - PubMed
-
- Lederer DJ, Enright PL, Kawut SM, Hoffman EA, Hunninghake G, van Beek EJ, Austin JH, Jiang R, Lovasi GS, Barr RG. Cigarette smoking is associated with subclinical parenchymal lung disease: the Multi-Ethnic Study of Atherosclerosis (MESA)-lung study. Am J Respir Crit Care Med. 2009;180(5):407–414. - PMC - PubMed
-
- Tsushima K, Sone S, Yoshikawa S, Yokoyama T, Suzuki T, Kubo K. The radiological patterns of interstitial change at an early phase: over a 4-year follow-up. Respiratory medicine. 2010;104(11):1712–1721. - PubMed
-
- Araki T, Putman RK, Hatabu H, Gao W, Dupuis J, Latourelle JC, Nishino M, Zazueta OE, Kurugol S, Ross JC, San Jose Estepar R, Schwartz DA, Rosas IO, Washko GR, O’Connor GT, Hunninghake GM. Development and Progression of Interstitial Lung Abnormalities in the Framingham Heart Study. Am J Respir Crit Care Med. 2016 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL113264/HL/NHLBI NIH HHS/United States
- T32 HL007633/HL/NHLBI NIH HHS/United States
- N01 AG012100/AG/NIA NIH HHS/United States
- R01 HL130974/HL/NHLBI NIH HHS/United States
- R01 HL130275/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- R01 HL135142/HL/NHLBI NIH HHS/United States
- R01 HL118455/HL/NHLBI NIH HHS/United States
- R33 HL120794/HL/NHLBI NIH HHS/United States
- I01 BX001534/BX/BLRD VA/United States
- K25 HL130637/HL/NHLBI NIH HHS/United States
- R01 HL097163/HL/NHLBI NIH HHS/United States
- R33 HL120770/HL/NHLBI NIH HHS/United States
- R25 ES025476/ES/NIEHS NIH HHS/United States
- K25 HL104085/HL/NHLBI NIH HHS/United States
- P01 HL114501/HL/NHLBI NIH HHS/United States
- R01 HL122464/HL/NHLBI NIH HHS/United States
- R01 HL089897/HL/NHLBI NIH HHS/United States
- P01 HL092870/HL/NHLBI NIH HHS/United States
- UH2 HL123442/HL/NHLBI NIH HHS/United States
- U19 AI095219/AI/NIAID NIH HHS/United States
- HHSN271201200022C/AG/NIA NIH HHS/United States
- R01 HL111024/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- P01 HL132825/HL/NHLBI NIH HHS/United States
- R01 HL129920/HL/NHLBI NIH HHS/United States
- R01 HL123546/HL/NHLBI NIH HHS/United States
- K23 CA157631/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials