

Bilateral Hydroureteronephrosis with a Hypertrophied, Trabeculated Urinary Bladder
- PMID: 28894411
- PMCID: PMC5566069
- DOI: 10.21315/mjms2017.24.2.14
Bilateral Hydroureteronephrosis with a Hypertrophied, Trabeculated Urinary Bladder
Abstract
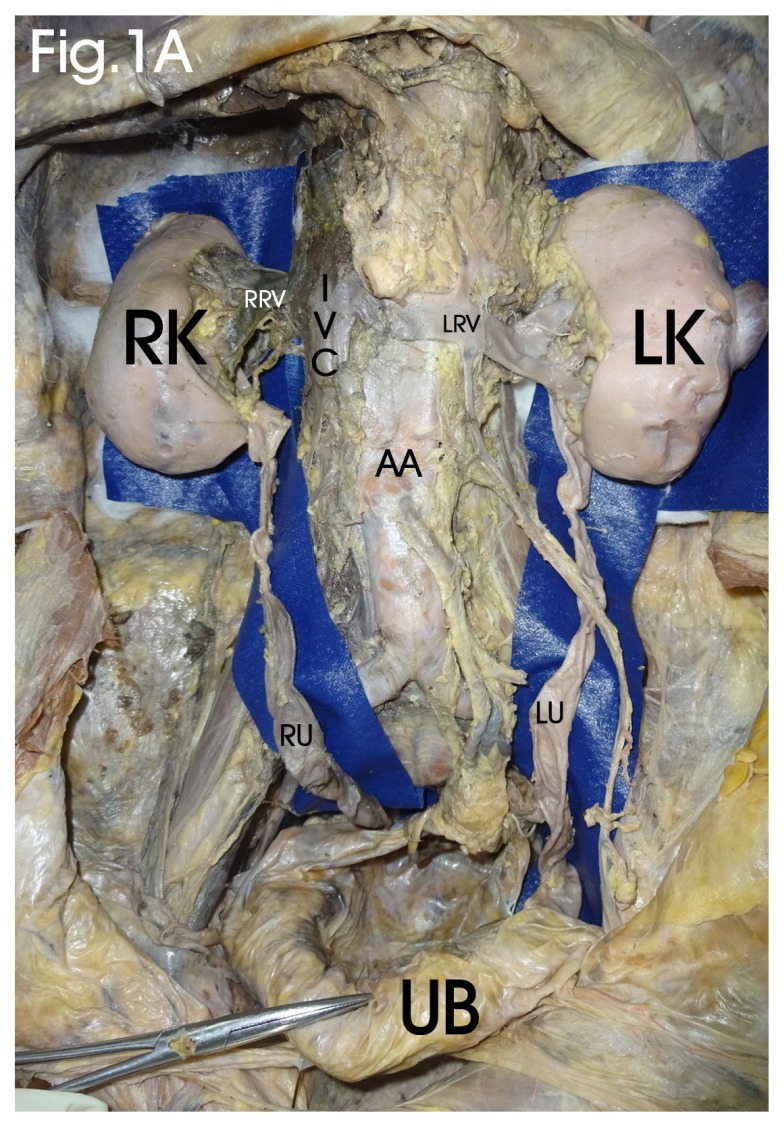
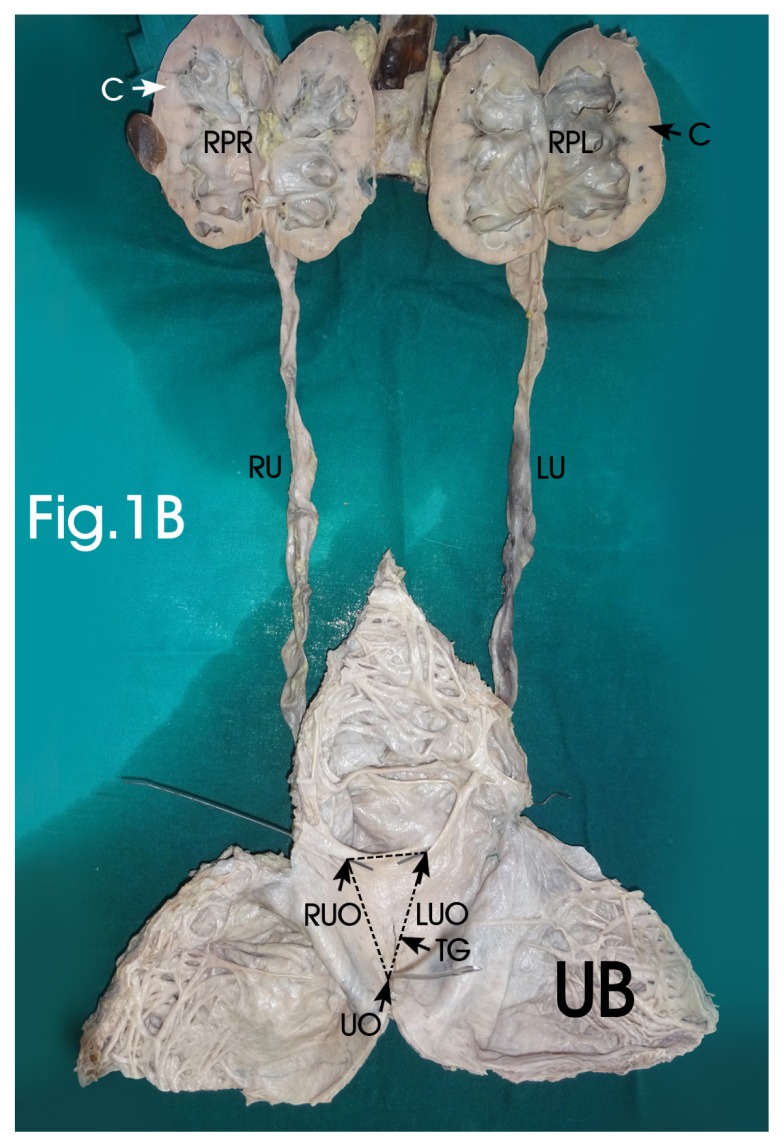
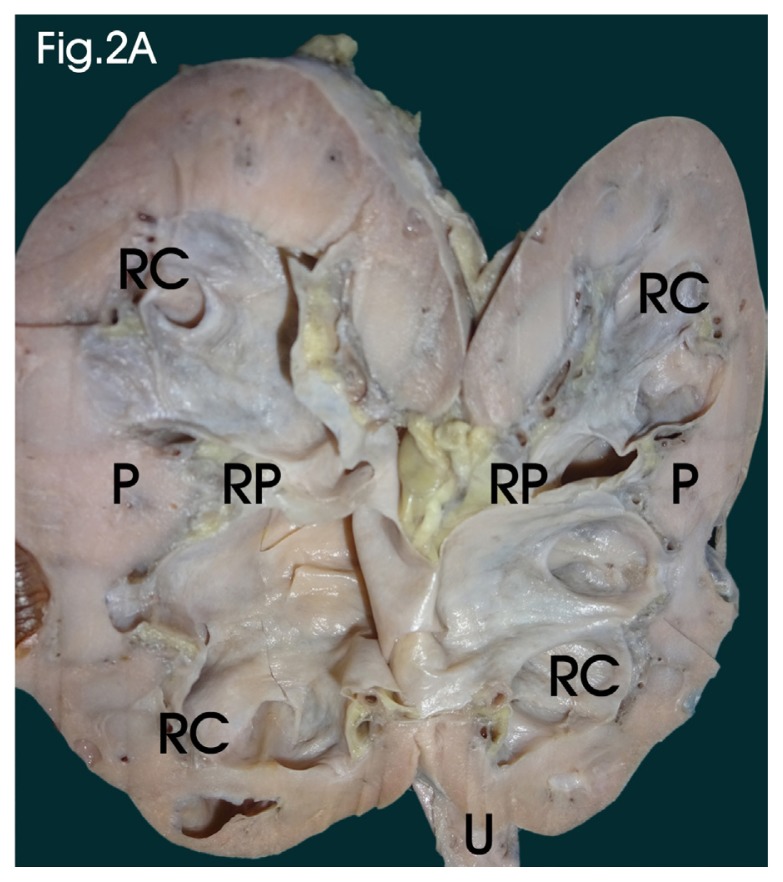
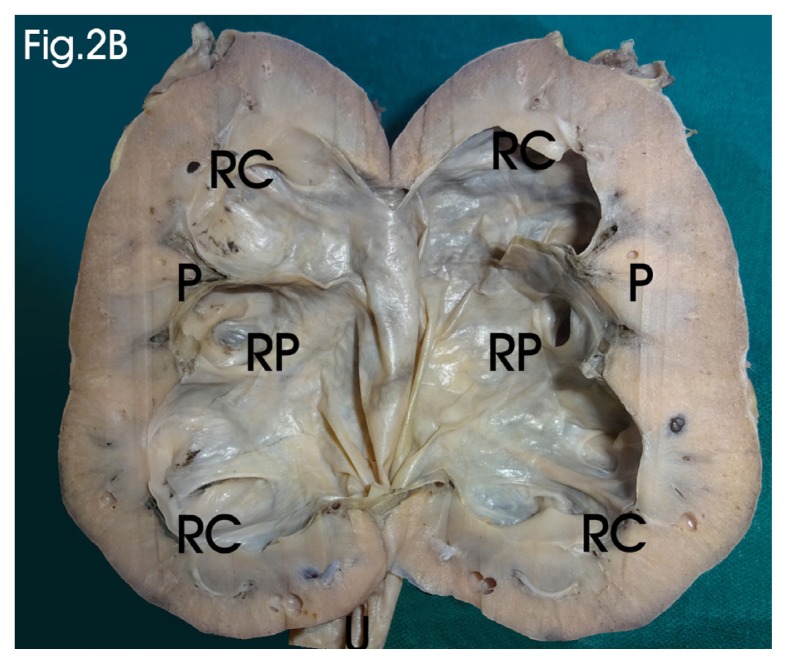
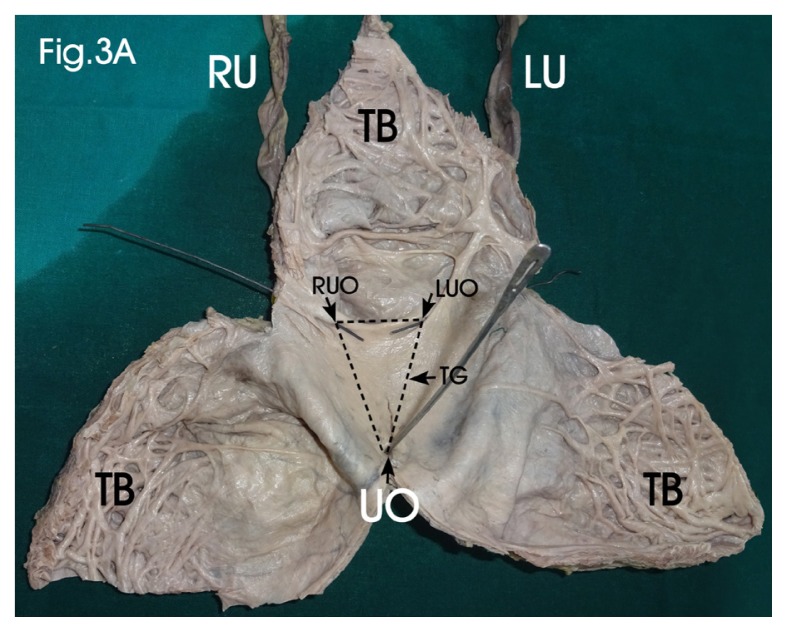
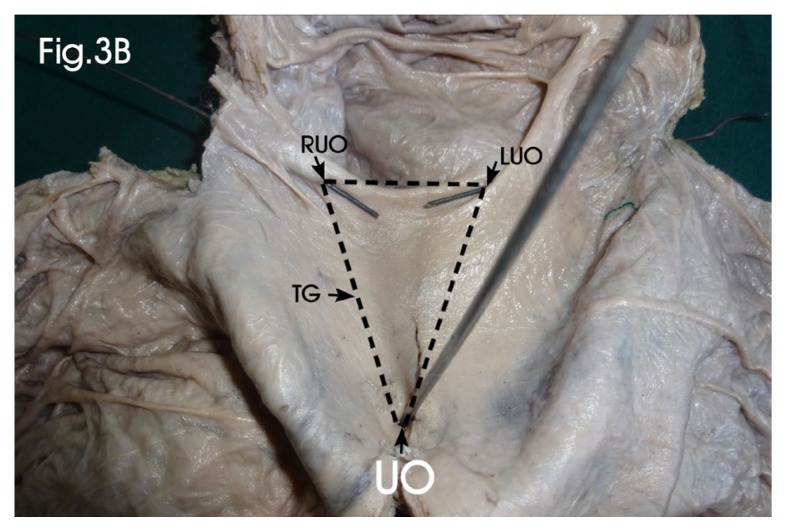
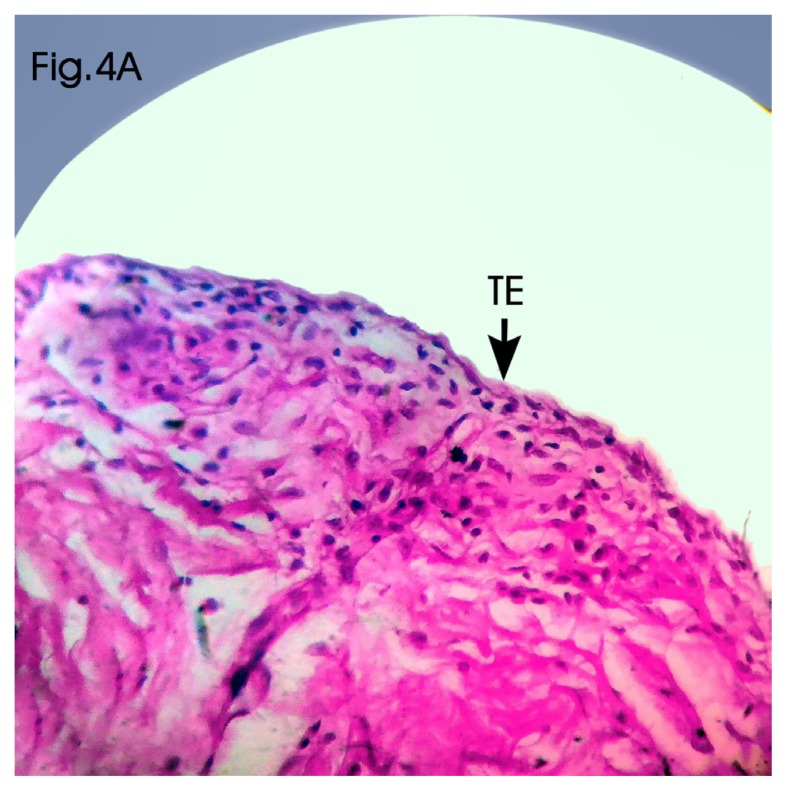
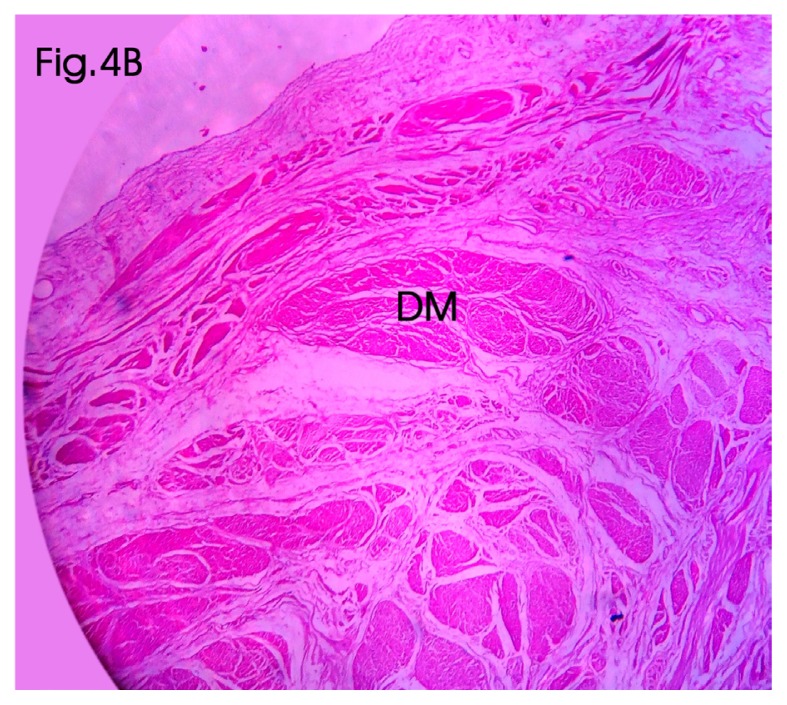
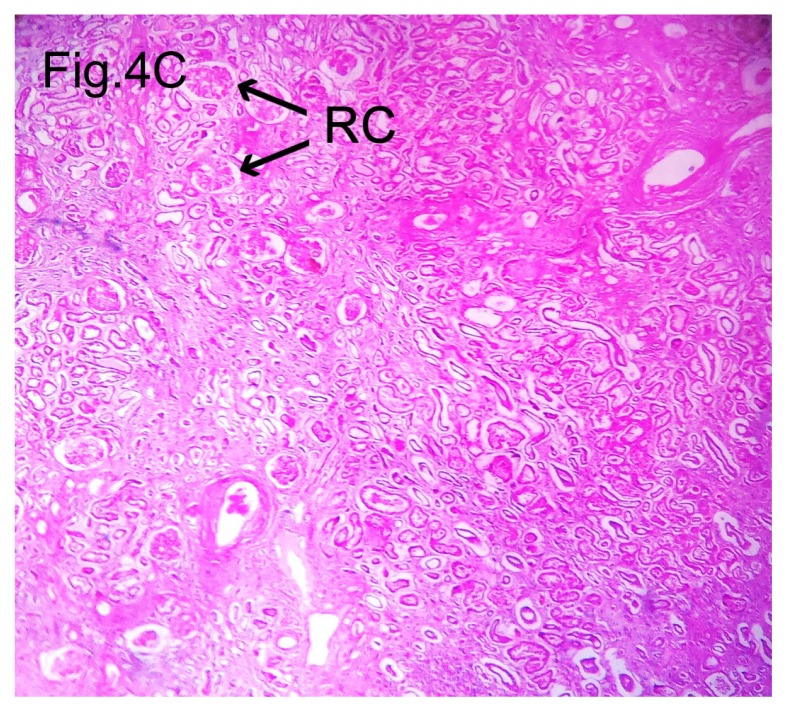
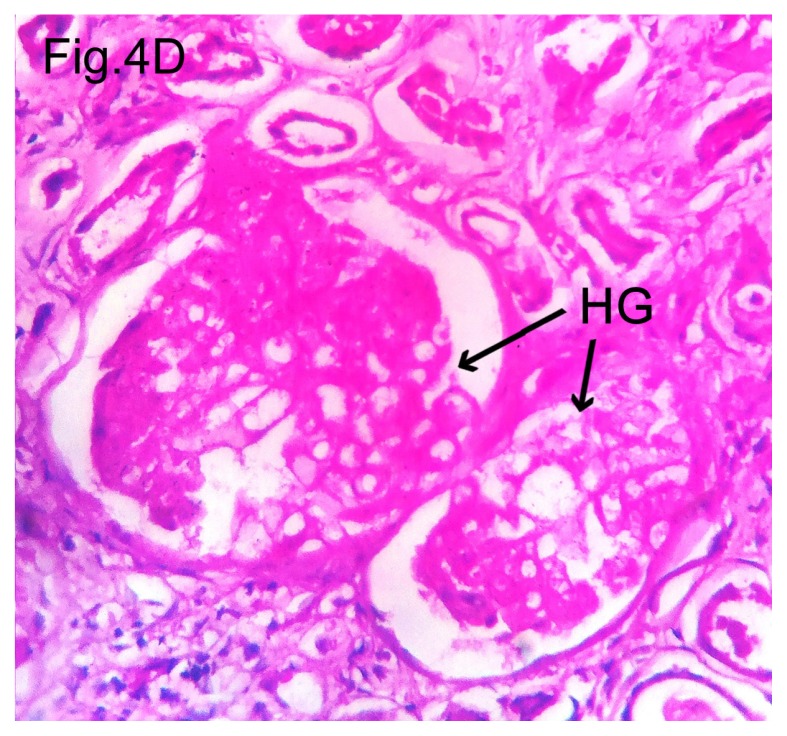
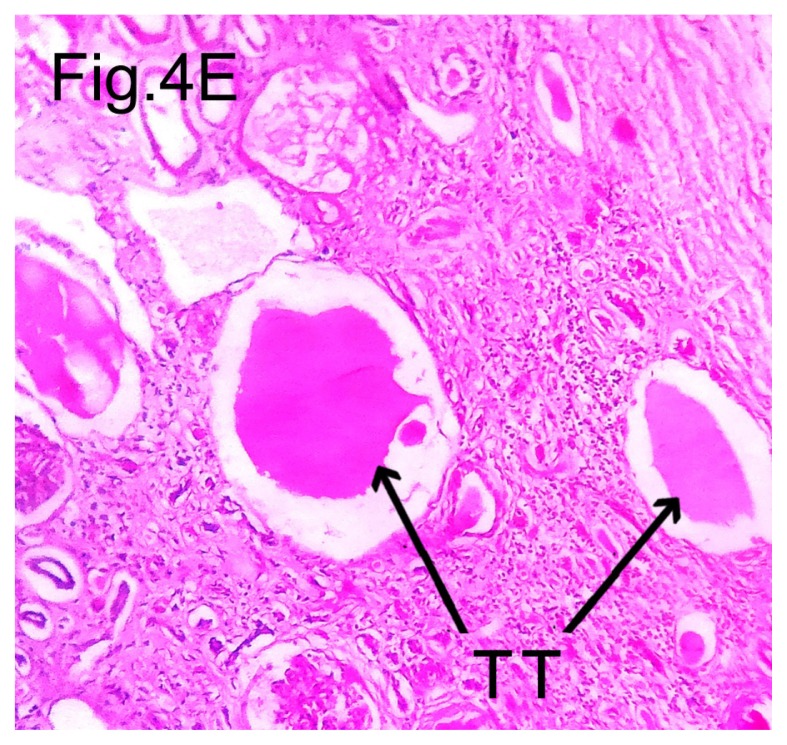
Bilateral hydroureteronephrosis involves the dilatation of the renal pelvis, calyces and ureter; it develops secondary to urinary tract obstruction and leads to a build-up of back pressure in the urinary tract, and it may lead to impairment of renal function and ultimately culminate in renal failure. Although clinically silent in most cases, it can be diagnosed as an incidental finding during evaluation of an unrelated cause. In a minority of patients, it presents with signs and symptoms. Renal calculus is the most common cause, but there are multiple non-calculus aetiologies, and they depend on age and sex. Pelviureteric junction obstruction, benign prostatic hypertrophy, urethral stricture, neurogenic bladder, retroperitoneal mass and bladder outlet obstruction are some of the frequent causes of hydroureteronephrosis in adults. The incidence of non-calculus hydronephrosis is more common in males than in females. Ultrasonography is the most important baseline investigation in the evaluation of patients with hydronephrosis. Here, we report a rarely seen case of bilateral hydroureteronephrosis associated with a hypertrophied, trabeculated bladder in an adult male cadaver, suspected to be due to a primary bladder neck obstruction, and analyse its various other causes, clinical presentations and outcomes.
Keywords: hydronephrosis; prostatic hyperplasia; ultrasonography; urinary bladder neck obstruction; urodynamics.
Conflict of interest statement
Conflicts of Interest None
Figures
References
-
- Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran pathologic basis of disease. 8th ed. Philadelphia PA: Elsevier Saunders; 2010. pp. 960–962.
-
- Mergener K, Weinerth JL, Baillie J. Dietl’s crisis: a syndrome of episodic abdominal pain of urologic origin that may present to a gastroenterologist. Am J Gastroenterol. 1997;92(12):2289–2291. - PubMed
-
- Merck Manuals Home Health Handbook. Hydronephrosis. (cited 2010 Nov 5) Available from: http://www.merckmanuals.com/home/index.html.
-
- Lameire N, Van Biesen W, Vanholder R. Acute renal failure. Lancet. 2005;365:417–430. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources