

Current Diagnosis and Management of Cervical Spondylotic Myelopathy
- PMID: 28894688
- PMCID: PMC5582708
- DOI: 10.1177/2192568217699208
Current Diagnosis and Management of Cervical Spondylotic Myelopathy
Abstract
Study design: Review.
Objectives: Cervical spondylotic myelopathy (CSM) is a major cause of disability, particular in elderly patients. Awareness and understanding of CSM is imperative to facilitate early diagnosis and management. This review article addresses CSM with regard to its epidemiology, anatomical considerations, pathophysiology, clinical manifestations, imaging characteristics, treatment approaches and outcomes, and the cost-effectiveness of surgical options.
Methods: The authors performed an extensive review of the peer-reviewed literature addressing the aforementioned objectives.
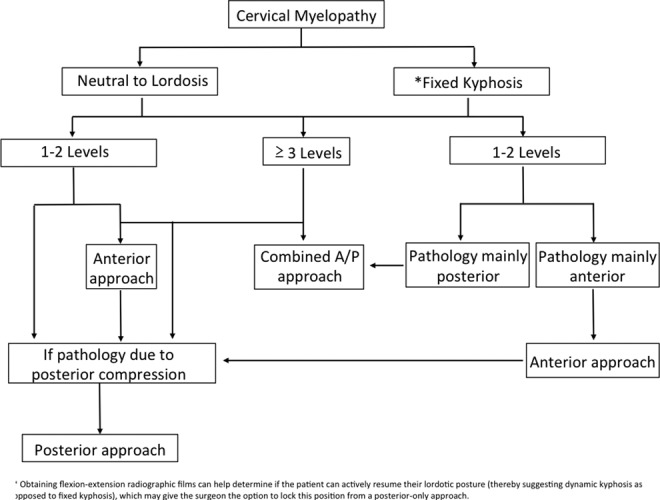
Results: The clinical presentation and natural history of CSM is variable, alternating between quiescent and insidious to stepwise decline or rapid neurological deterioration. For mild CSM, conservative options could be employed with careful observation. However, surgical intervention has shown to be superior for moderate to severe CSM. The success of operative or conservative management of CSM is multifactorial and high-quality studies are lacking. The optimal surgical approach is still under debate, and can vary depending on the number of levels involved, location of the pathology and baseline cervical sagittal alignment.
Conclusions: Early recognition and treatment of CSM, before the onset of spinal cord damage, is essential for optimal outcomes. The goal of surgery is to decompress the cord with expansion of the spinal canal, while restoring cervical lordosis, and stabilizing when the risk of cervical kyphosis is high. Further high-quality randomized clinical studies with long-term follow up are still needed to further define the natural history and help predict the ideal surgical strategy.
Keywords: anterior cervical discectomy and fusion; cervical disk replacement; cervical laminoplasty; cervical spine stenosis; cervical spondylosis; cervical spondylotic myelopathy; degenerative disc disease.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Singh A, Tetreault L, Casey A, Laing R, Statham P, Fehlings MG. A summary of assessment tools for patients suffering from cervical spondylotic myelopathy: a systematic review on validity, reliability and responsiveness. Eur Spine J. 2015;24(suppl 2):209–228. doi:10.1007/s00586-013-2935-x. - PubMed
-
- Edwards CC, 2nd, Riew KD, Anderson PA, Hilibrand AS, Vaccaro AF. Cervical myelopathy. current diagnostic and treatment strategies. Spine J. 2003;3:68–81. - PubMed
-
- Klineberg E. Cervical spondylotic myelopathy: a review of the evidence. Orthop Clin North Am. 2010;41:193–202. doi:10.1016/j.ocl.2009.12.010. - PubMed
-
- Lad SP, Patil CG, Berta S, Santarelli JG, Ho C, Boakye M. National trends in spinal fusion for cervical spondylotic myelopathy. Surg Neurol. 2009;71:66–69. doi:10.1016/j.surneu.2008.02.045. - PubMed
-
- Wu JC, Ko CC, Yen YS, et al. Epidemiology of cervical spondylotic myelopathy and its risk of causing spinal cord injury: a national cohort study. Neurosurg Focus. 2013;35:E10 doi:10.3171/2013.4.FOCUS13122. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
