

Treatment of the Enlarged Clitoris
- PMID: 28894728
- PMCID: PMC5581357
- DOI: 10.3389/fped.2017.00125
Treatment of the Enlarged Clitoris
Abstract
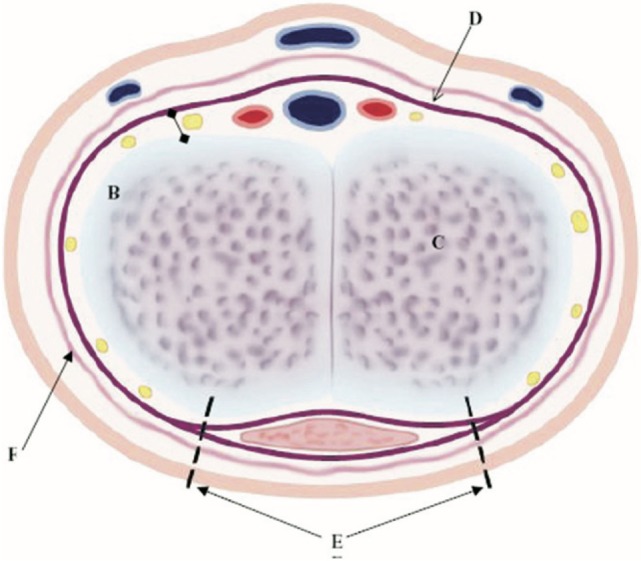
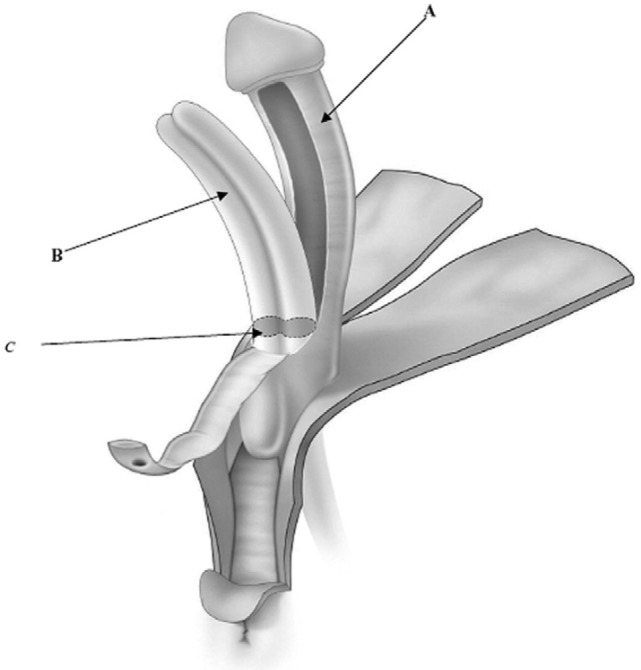
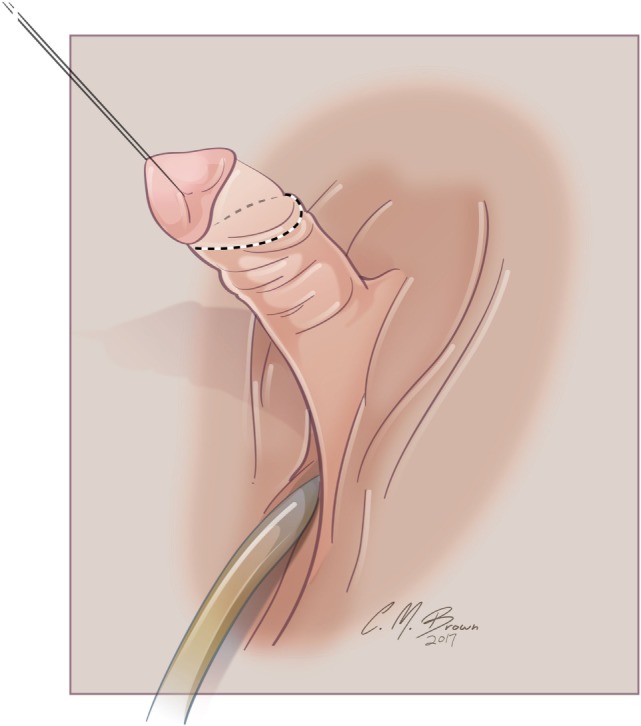
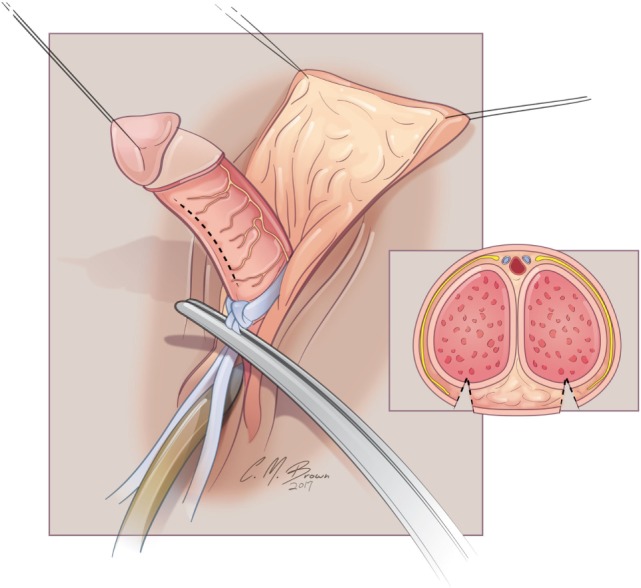
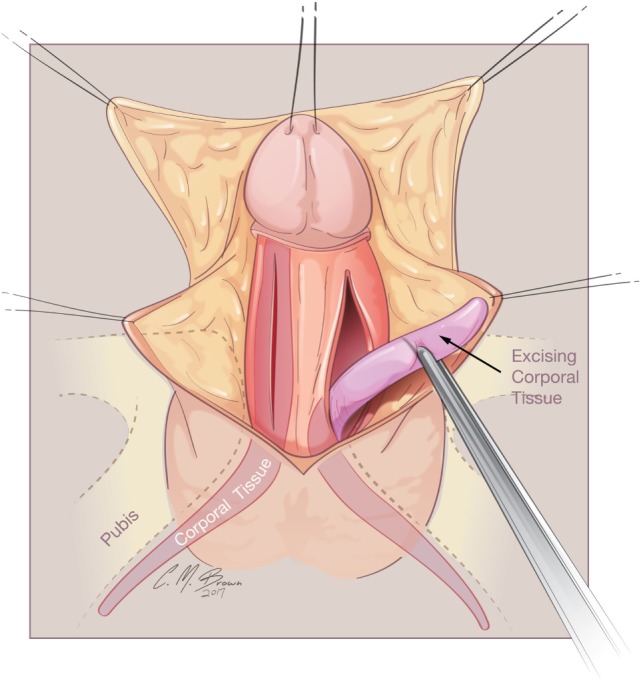
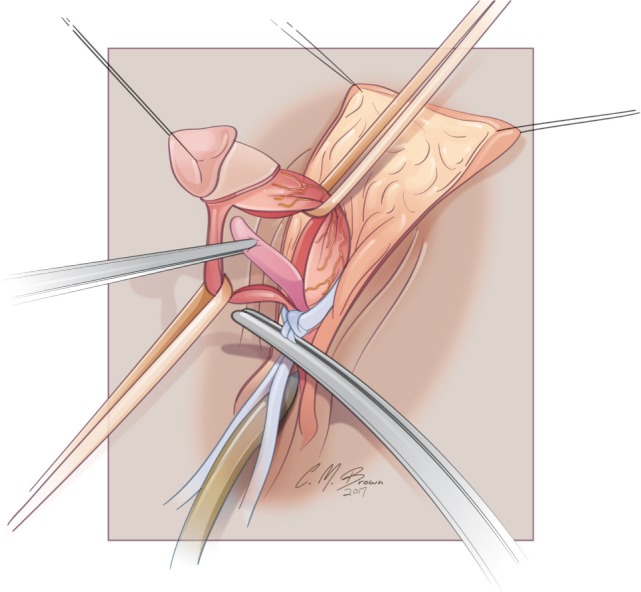
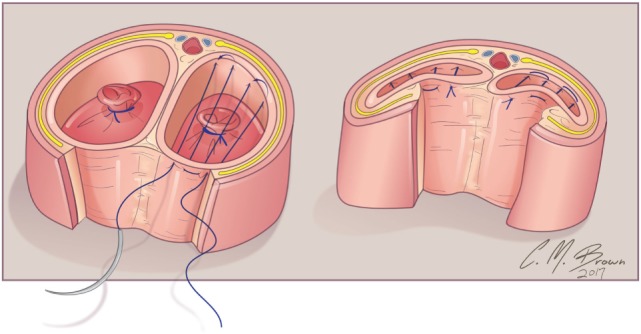
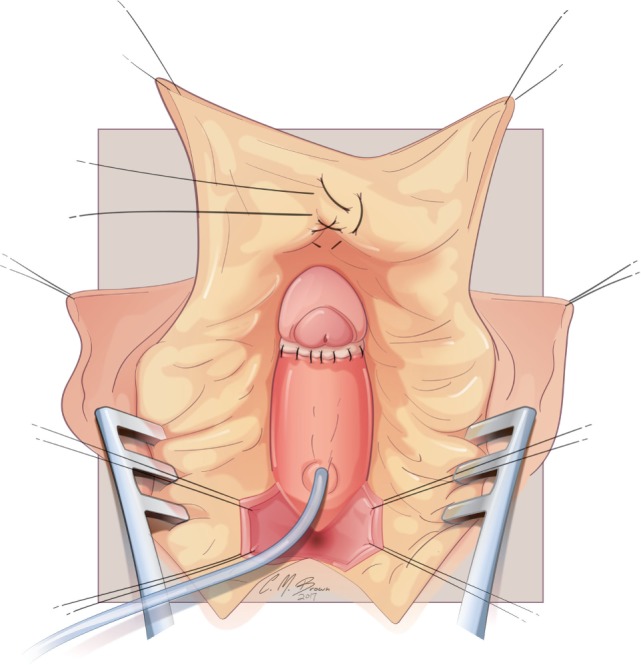
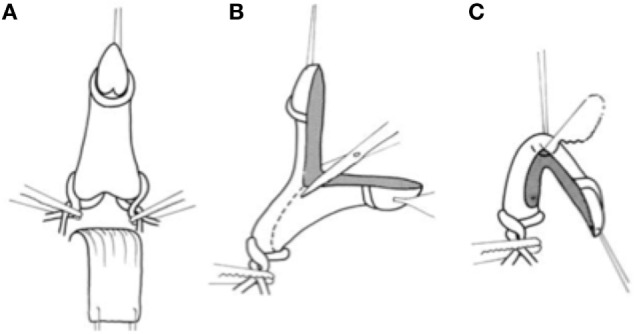
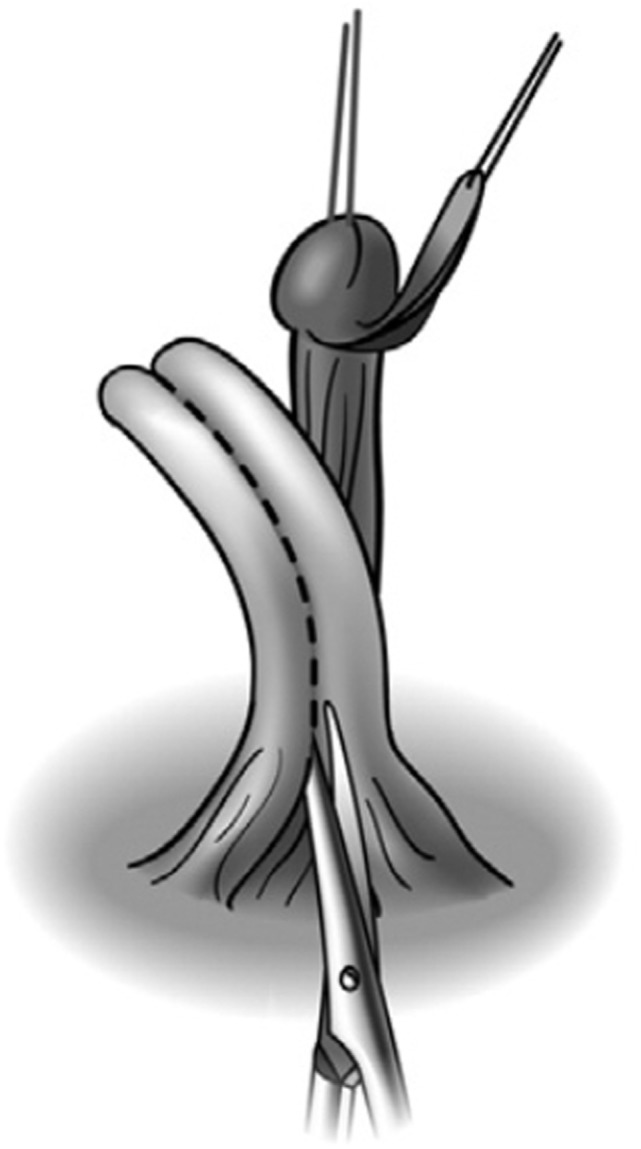
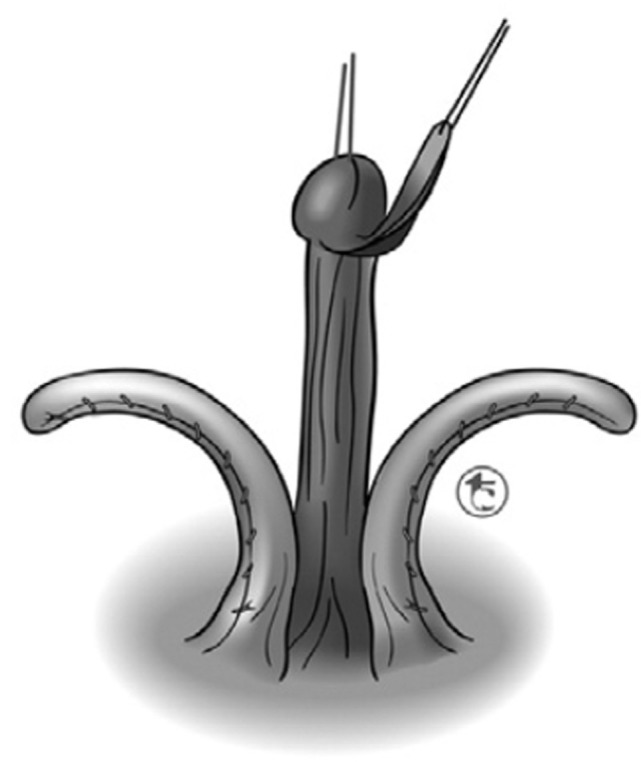
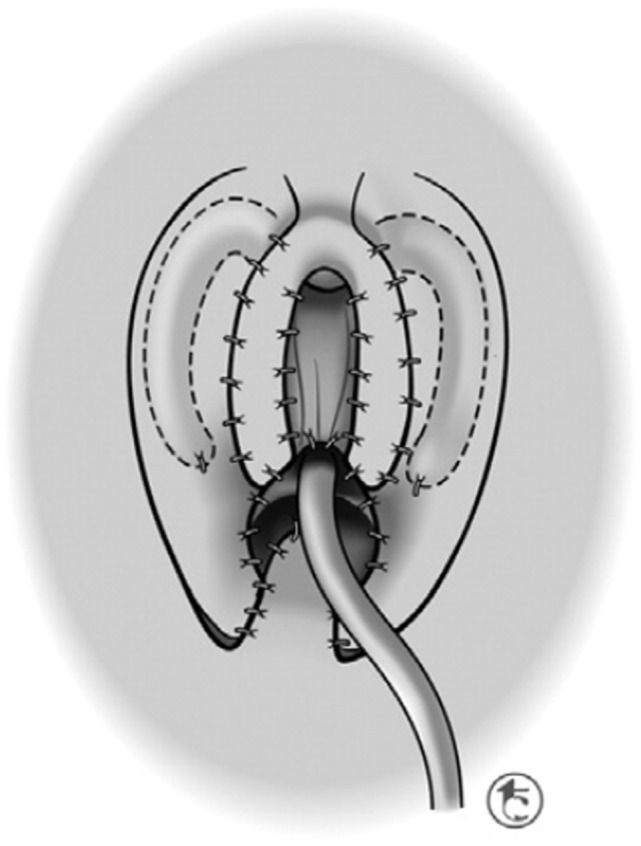
Management of the enlarged clitoris, because of its import for sexual function, has been and remains one of the most controversial topics in pediatric urology. Early controversy surrounding clitoroplasty resulted from many factors including an incomplete understanding of clitoral anatomy and incorrect assumptions of the role of the clitoris in sexual function. With a better understanding of anatomy and function, procedures have evolved to preserve clitoral tissue, especially with respect to the neurovascular bundles. These changes have been made in an effort to preserve clitoral sensation and preserve orgasmic potential. It is the goal of this manuscript to describe the different procedures that have been developed for the surgical management of clitoromegally, with emphasis on the risks and benefits of each. Equally important to any discussion of such a sensitive topic is an understanding of long-term patient outcomes. As we will see, despite its importance, there has been a dearth of data in this regard. Future work in the arena of patient satisfaction will undoubtedly play a major role in directing our surgical approach.
Keywords: clitoromegally; clitoroplasty; congenital adrenal hyperplasia; disorders of sex development; history.
Figures
References
-
- O’Connell HE, Sanjeevan KV, Hutson JM. Anatomy of the clitoris. J Urol (2005) 174:1189. 10.1097/01.ju.0000173639.38898.cd - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials