

Factors affecting revision rate of chronic rhinosinusitis
- PMID: 28894807
- PMCID: PMC5510254
- DOI: 10.1002/lio2.27
Factors affecting revision rate of chronic rhinosinusitis
Abstract
Objective: Chronic rhinosinusitis (CRS) is a variable multifactorial disease. It can be divided into forms with nasal polyps (CRSwNP) and without (CRSsNP). Sinus and/or nasal polypectomy surgery are considered if maximal conservative treatment is insufficient. The predictive factors of the need of revision surgery comprise mostly the CRSwNP phenotype and are not fully understood.
Study design: The aim of this follow-up study was to evaluate the factors associated with the revision surgery rate in CRS patients with variable extent of disease.
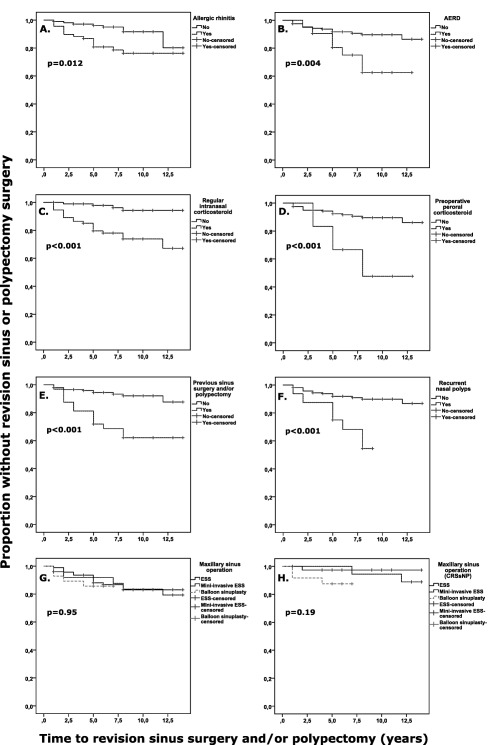
Methods: Data of CRS patients (N = 178) undergoing sinus surgery and/or nasal polypectomy in 2001 to 2010 were used. Patient characteristics and follow-up data were collected from patient records and questionnaires. Associations were analyzed by Fisher's exact, Mann Whitney U, and the Kaplan-Meier method with log-rank test. Unadjusted Cox's proportional hazard models were used for 12 variables and were fitted for the need for revision sinus surgery and/or nasal polypectomy during follow-up of in average 9 years.
Results: The proportion of CRS patients who had undergone revision in 5 years was 9.6%. After adjustment, the following factors associated significantly with the need for recurrent CRS surgery: allergic rhinitis, corticosteroid treatment, previous surgery of CRS, and recurrent NP.
Conclusion: Increased risk of progressive CRS phenotypes with the need for revision surgery would putatively be recognized by relatively simple clinical questions. Further studies with increased sample size are needed to evaluate whether these predictive factors would be relevant for developing better detection and management of progressive CRS.
Level of evidence: 2b.
Keywords: Antrochoanal polyp; aspirin intolerance; aspirin‐exacerbated respiratory disease; inflammation; nasal polyp; recurrence; revision surgery; sinus surgery; sinusitis.
Figures

References
-
- Fokkens WJ, Lund VJ, Mullol J, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol Suppl 2012;3 p preceding table of contents, 1–298. - PubMed
-
- Hastan D, Fokkens WJ, Bachert C, et al. Chronic rhinosinusitis in Europe—an underestimated disease. A GA(2)LEN study. Allergy 2011;66:1216–1223. - PubMed
-
- Kim YS, Kim NH, Seong SY, Kim KR, Lee GB, Kim KS. Prevalence and risk factors of chronic rhinosinusitis in Korea. Am J Rhinol Allergy 2011;25:117–121. - PubMed
-
- Pilan RR, Pinna FR, Bezerra TF, et al. Prevalence of chronic rhinosinusitis in Sao Paulo. Rhinology 2012;50:129–138. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous