

Emerging insights into recurrent and metastatic human papillomavirus-related oropharyngeal squamous cell carcinoma
- PMID: 28894817
- PMCID: PMC5510283
- DOI: 10.1002/lio2.37
Emerging insights into recurrent and metastatic human papillomavirus-related oropharyngeal squamous cell carcinoma
Abstract
Objective: To review recent literature on human papillomavirus-related (HPV-positive) oropharyngeal squamous cell carcinoma (OPC) and focus on implications of recurrent and metastatic disease.
Methods: Primary articles from 1990 to 2016 indexed in MEDLINE (1) pertaining to the epidemiology of HPV-positive OPC and (2) providing clinical insight into recurrent and metastatic OPC.
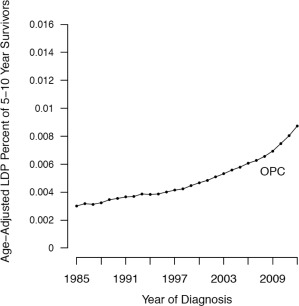
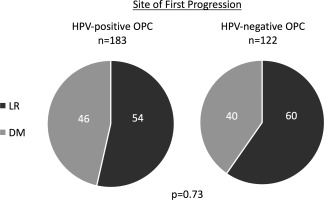
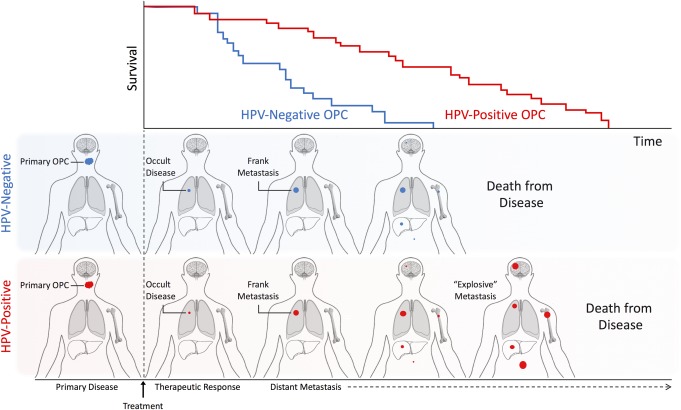
Results: The incidence of HPV-positive OPC is increasing globally. HPV-positive OPC is a subtype with distinct molecular and clinical features including enhanced treatment response and improved overall survival. While disease recurrence is less common in patients with HPV-positive OPC, up to 36% of patients experience treatment failure within eight years. Recurrent and metastatic OPC has historically signified poor prognosis, however recent data are challenging this dogma. Here, we discuss recurrent and metastatic OPC in the context of HPV tumor status.
Conclusion: HPV-positive OPC exhibits distinct genetic, cellular, epidemiological, and clinical features from HPV-negative OPC. HPV tumor status is emerging as a marker indicative of improved prognosis after disease progression in both locoregionally recurrent and distant metastatic OPC.
Level of evidence: N/A.
Keywords: HNSCC; HPV; Head and neck; OPSCC; human papillomavirus; metastatic; oropharyngeal; prognosis; recurrent; squamous cell carcinoma; survival.
Figures
References
-
- American Joint Committee on Cancer (AJCC) . AJCC Cancer Staging Manual. 7th Ed Chicago, IL: Springer, 2010.
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International journal of cancer 2015; 136:E359–386. - PubMed
-
- Satterwhite CL, Torrone E, Meites E, et al. Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. Sex Transm Dis 2013;40:187–193. - PubMed
-
- D'Souza G, Kreimer AR, Viscidi R, et al. Case‐control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 2007;356:1944–1956. - PubMed
-
- Gillison ML, Koch WM, Capone RB, et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 2000;92:709–720. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials