

Projecting social contact matrices in 152 countries using contact surveys and demographic data
- PMID: 28898249
- PMCID: PMC5609774
- DOI: 10.1371/journal.pcbi.1005697
Projecting social contact matrices in 152 countries using contact surveys and demographic data
Abstract
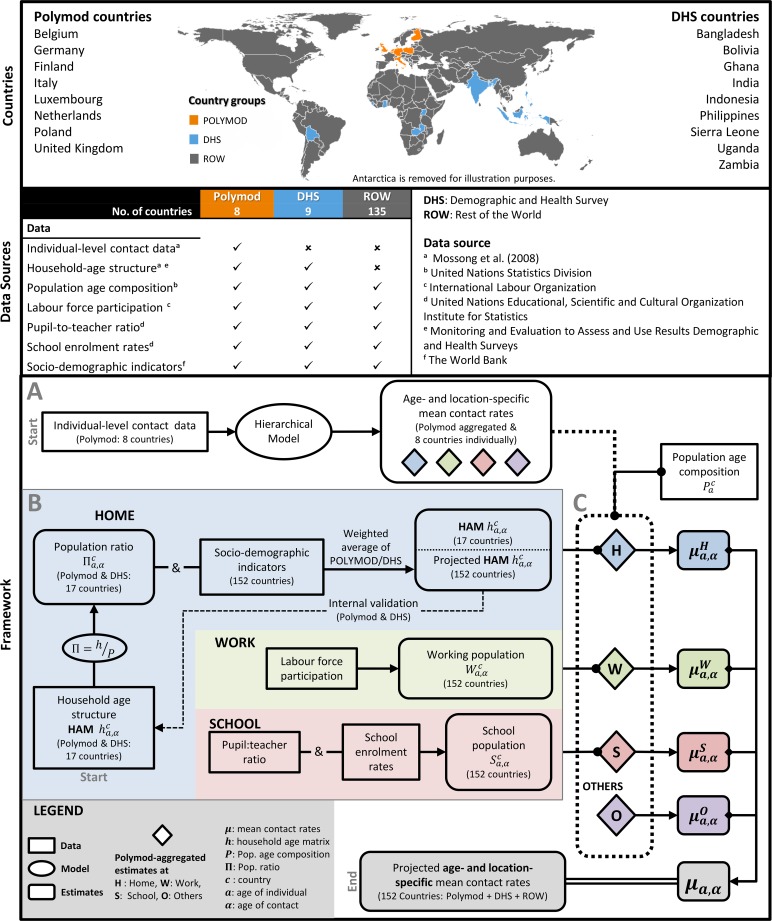
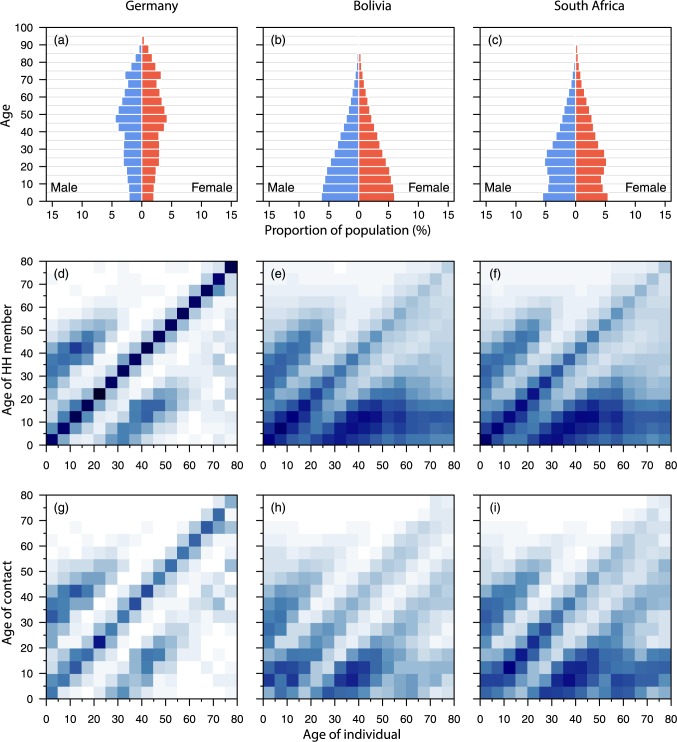
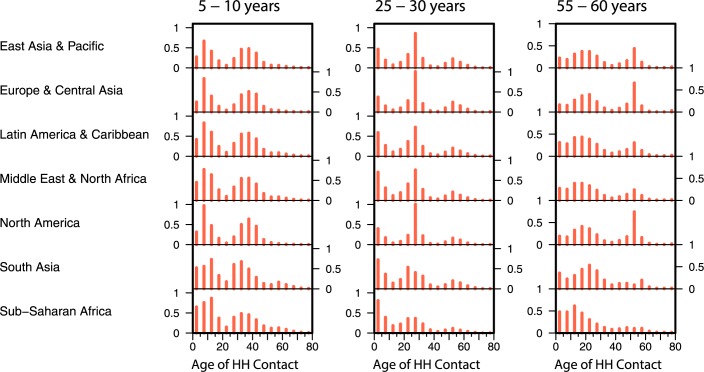
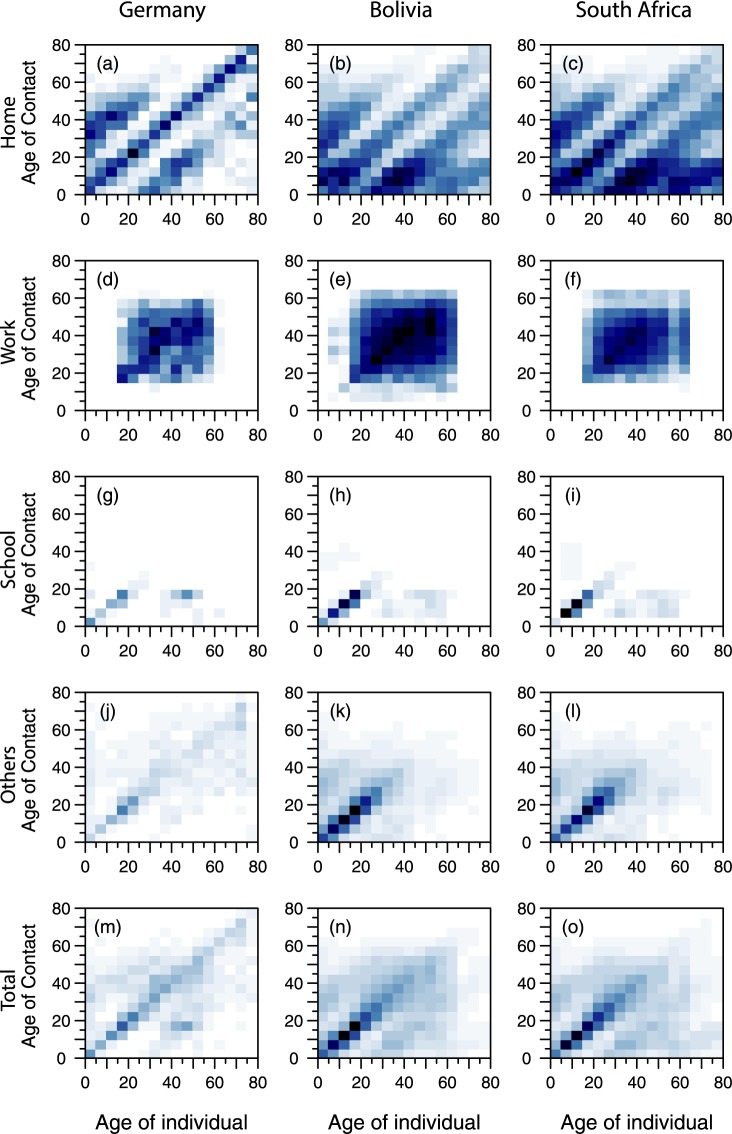
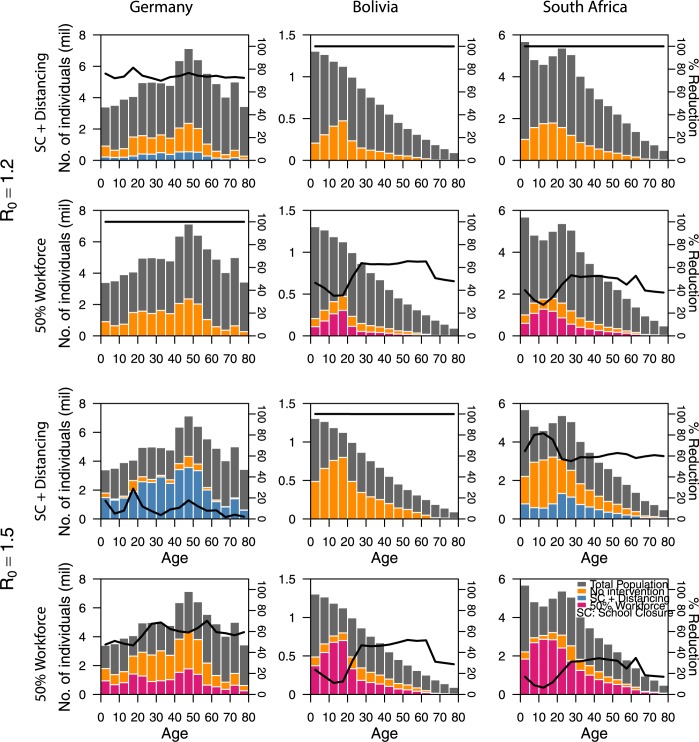
Heterogeneities in contact networks have a major effect in determining whether a pathogen can become epidemic or persist at endemic levels. Epidemic models that determine which interventions can successfully prevent an outbreak need to account for social structure and mixing patterns. Contact patterns vary across age and locations (e.g. home, work, and school), and including them as predictors in transmission dynamic models of pathogens that spread socially will improve the models' realism. Data from population-based contact diaries in eight European countries from the POLYMOD study were projected to 144 other countries using a Bayesian hierarchical model that estimated the proclivity of age-and-location-specific contact patterns for the countries, using Markov chain Monte Carlo simulation. Household level data from the Demographic and Health Surveys for nine lower-income countries and socio-demographic factors from several on-line databases for 152 countries were used to quantify similarity of countries to estimate contact patterns in the home, work, school and other locations for countries for which no contact data are available, accounting for demographic structure, household structure where known, and a variety of metrics including workforce participation and school enrolment. Contacts are highly assortative with age across all countries considered, but pronounced regional differences in the age-specific contacts at home were noticeable, with more inter-generational contacts in Asian countries than in other settings. Moreover, there were variations in contact patterns by location, with work-place contacts being least assortative. These variations led to differences in the effect of social distancing measures in an age structured epidemic model. Contacts have an important role in transmission dynamic models that use contact rates to characterize the spread of contact-transmissible diseases. This study provides estimates of mixing patterns for societies for which contact data such as POLYMOD are not yet available.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Sabanathan S, Tan LV, Thwaites L, Wills B, Qui PT, Rogier van Doorn H. Enterovirus 71 related severe hand, foot and mouth disease outbreaks in South-East Asia: current situation and ongoing challenges. J Epidemiol Community Health. 2014;68: 500–502. doi: 10.1136/jech-2014-203836 - DOI - PMC - PubMed
-
- Koh WM, Bogich T, Siegel K, Jin J, Chong EY, Tan CY, et al. The Epidemiology of Hand, Foot and Mouth Disease in Asia: A Systematic Review and Analysis. Pediatr Infect Dis J. 2016;35: e285–e300. doi: 10.1097/INF.0000000000001242 - DOI - PMC - PubMed
-
- Penttinen PM, Kaasik-Aaslav K, Friaux A, Donachie A, Sudre B, Amato-Gauci AJ, et al. Taking stock of the first 133 MERS coronavirus cases globally–Is the epidemic changing? Eurosurveillance. 2013;18 Available: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20596 - PubMed
-
- Gomes MFC, Pastore y Piontti A, Rossi L, Chao D, Longini I, Halloran ME, et al. Assessing the International Spreading Risk Associated with the 2014 West African Ebola Outbreak. PLoS Curr. 2014; doi: 10.1371/currents.outbreaks.cd818f63d40e24aef769dda7df9e0da5 - DOI - PMC - PubMed
-
- Khan K, Arino J, Hu W, Raposo P, Sears J, Calderon F, et al. Spread of a Novel Influenza A (H1N1) Virus via Global Airline Transportation. N Engl J Med. 2009;361: 212–214. doi: 10.1056/NEJMc0904559 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
