

Sustained effectiveness and cost-effectiveness of the Healthy Activity Programme, a brief psychological treatment for depression delivered by lay counsellors in primary care: 12-month follow-up of a randomised controlled trial
- PMID: 28898283
- PMCID: PMC5595303
- DOI: 10.1371/journal.pmed.1002385
Sustained effectiveness and cost-effectiveness of the Healthy Activity Programme, a brief psychological treatment for depression delivered by lay counsellors in primary care: 12-month follow-up of a randomised controlled trial
Abstract
Background: The Healthy Activity Programme (HAP), a brief behavioural intervention delivered by lay counsellors, enhanced remission over 3 months among primary care attendees with depression in peri-urban and rural settings in India. We evaluated the sustainability of the effects after treatment termination, the cost-effectiveness of HAP over 12 months, and the effects of the hypothesized mediator of activation on clinical outcomes.
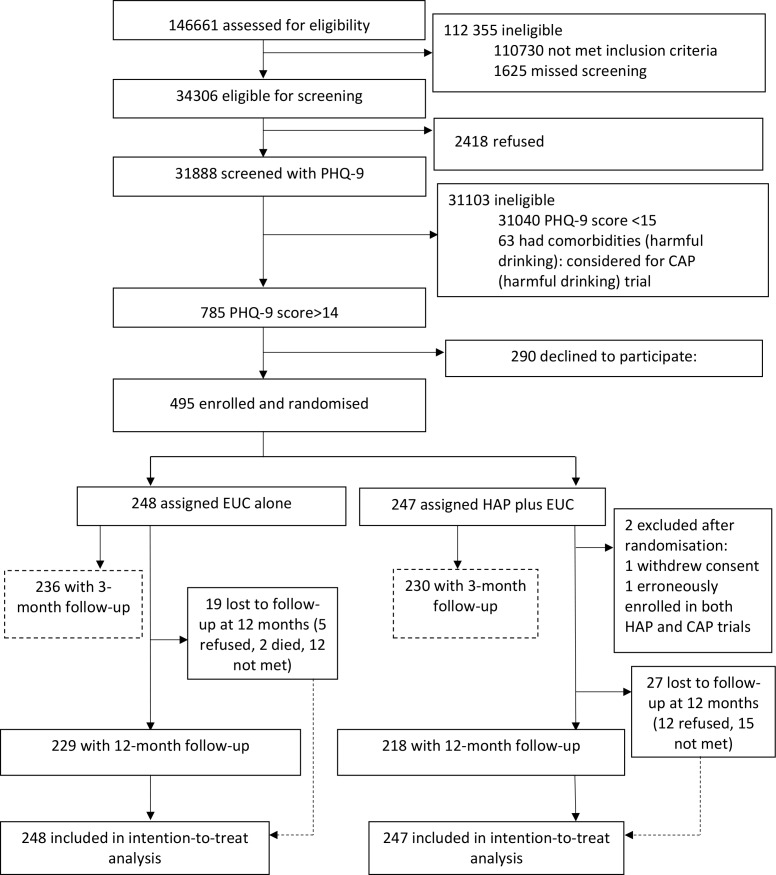
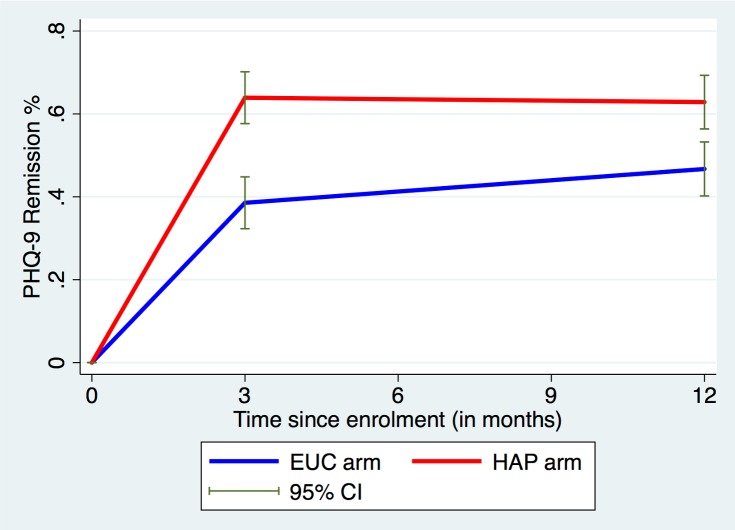
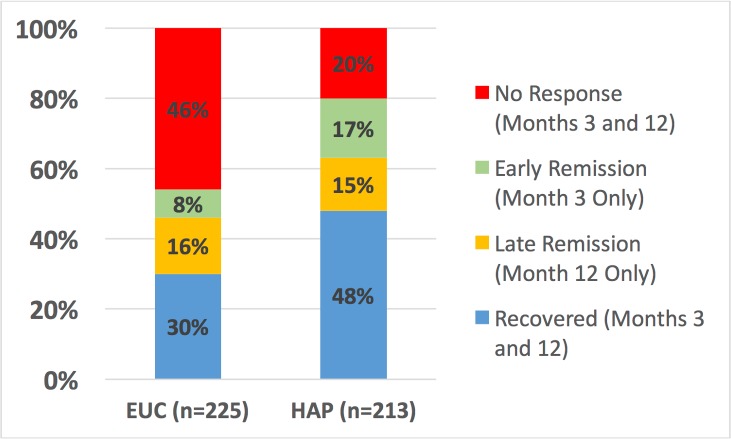
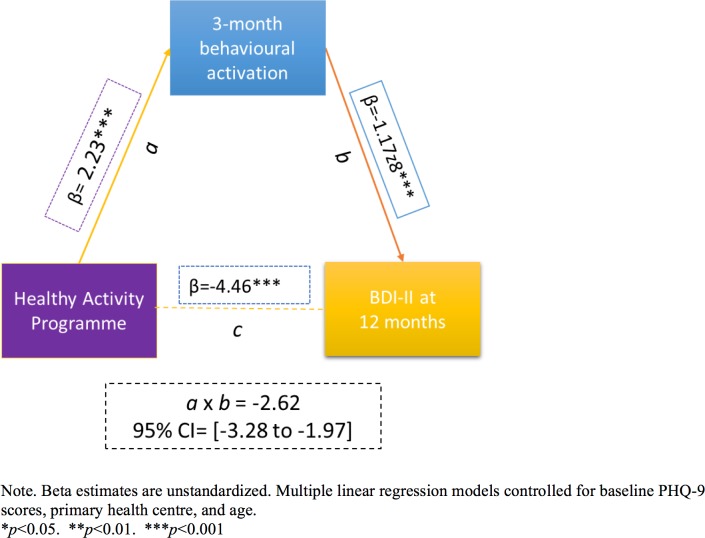
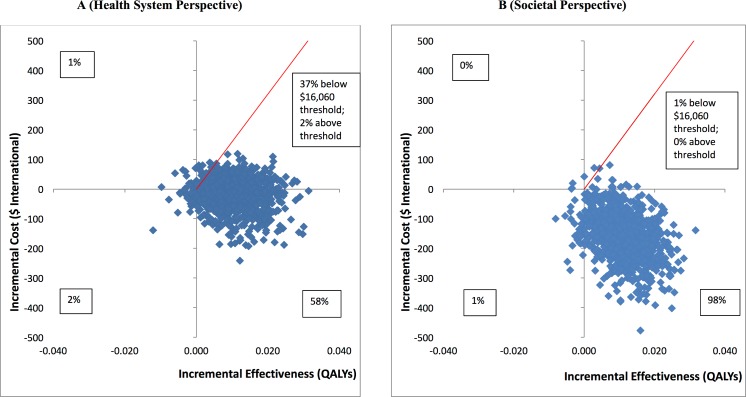
Methods and findings: Primary care attendees aged 18-65 years screened with moderately severe to severe depression on the Patient Health Questionnaire 9 (PHQ-9) were randomised to either HAP plus enhanced usual care (EUC) (n = 247) or EUC alone (n = 248), of whom 95% completed assessments at 3 months, and 91% at 12 months. Primary outcomes were severity on the Beck Depression Inventory-II (BDI-II) and remission on the PHQ-9. HAP participants maintained the gains they showed at the end of treatment through the 12-month follow-up (difference in mean BDI-II score between 3 and 12 months = -0.34; 95% CI -2.37, 1.69; p = 0.74), with lower symptom severity scores than participants who received EUC alone (adjusted mean difference in BDI-II score = -4.45; 95% CI -7.26, -1.63; p = 0.002) and higher rates of remission (adjusted prevalence ratio [aPR] = 1.36; 95% CI 1.15, 1.61; p < 0.009). They also fared better on most secondary outcomes, including recovery (aPR = 1.98; 95% CI 1.29, 3.03; p = 0.002), any response over time (aPR = 1.45; 95% CI 1.27, 1.66; p < 0.001), higher likelihood of reporting a minimal clinically important difference (aPR = 1.42; 95% CI 1.17, 1.71; p < 0.001), and lower likelihood of reporting suicidal behaviour (aPR = 0.71; 95% CI 0.51, 1.01; p = 0.06). HAP plus EUC also had a marginal effect on WHO Disability Assessment Schedule score at 12 months (aPR = -1.58; 95% CI -3.33, 0.17; p = 0.08); other outcomes (days unable to work, intimate partner violence toward females) did not statistically significantly differ between the two arms. Economic analyses indicated that HAP plus EUC was dominant over EUC alone, with lower costs and better outcomes; uncertainty analysis showed that from this health system perspective there was a 95% chance of HAP being cost-effective, given a willingness to pay threshold of Intl$16,060-equivalent to GDP per capita in Goa-per quality-adjusted life year gained. Patient-reported behavioural activation level at 3 months mediated the effect of the HAP intervention on the 12-month depression score (β = -2.62; 95% CI -3.28, -1.97; p < 0.001). Serious adverse events were infrequent, and prevalence was similar by arm. We were unable to assess possible episodes of remission and relapse that may have occurred between our outcome assessment time points of 3 and 12 months after randomisation. We did not account for or evaluate the effect of mediators other than behavioural activation.
Conclusions: HAP's superiority over EUC at the end of treatment was largely stable over time and was mediated by patient activation. HAP provides better outcomes at lower costs from a perspective covering publicly funded healthcare services and productivity impacts on patients and their families.
Trial registration: ISRCTN registry ISRCTN95149997.
Conflict of interest statement
DM has received honoraria for lectures not related to this work from Otsuka Pharmaceuticals, Janssen-Cilag, and H Lundbeck in the past 2 years. CGF holds a Principal Research Fellowship from the Wellcome Trust (046386). VP is a member of the Editorial Board of PLOS Medicine. All other authors declare no competing interests.
Figures
References
-
- Patel V, Chisholm D, Parikh R, Charlson FJ, Degenhardt L, Dua T, et al. Addressing the burden of mental, neurological, and substance use disorders: key messages from Disease Control Priorities, 3rd edition. Lancet. 2016;387(10028):1672–85. doi: 10.1016/S0140-6736(15)00390-6 - DOI - PubMed
-
- Whiteford HA, Ferrari AJ, Degenhardt L, Feigin V, Vos T. The global burden of mental, neurological and substance use disorders: an analysis from the Global Burden of Disease Study 2010. PLoS ONE. 2015;10(2):e0116820 doi: 10.1371/journal.pone.0116820 - DOI - PMC - PubMed
-
- Chisholm D, Sweeny K, Sheehan P, Rasmussen B, Smit F, Cuijpers P, et al. Scaling-up treatment of depression and anxiety: a global return on investment analysis. Lancet Psychiatry. 2016;3(5):415–24. doi: 10.1016/S2215-0366(16)30024-4 - DOI - PubMed
-
- Gururaj G, Varghese M, Benegal V, Rao G, Pathak K, Singh L, et al. National Mental Health Survey of India, 2015–16: summary. Bengaluru: National Institute of Mental Health and Neurosciences; 2016. NIMHANS Publication No. 128.
-
- World Health Organization. mhGAP Mental Health Gap Action Programme: scaling up care for mental, neurological and substance use disorders. Geneva: World Health Organization; 2008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
