

Cancer of childhood in sub-Saharan Africa
- PMID: 28900468
- PMCID: PMC5574662
- DOI: 10.3332/ecancer.2017.755
Cancer of childhood in sub-Saharan Africa
Abstract
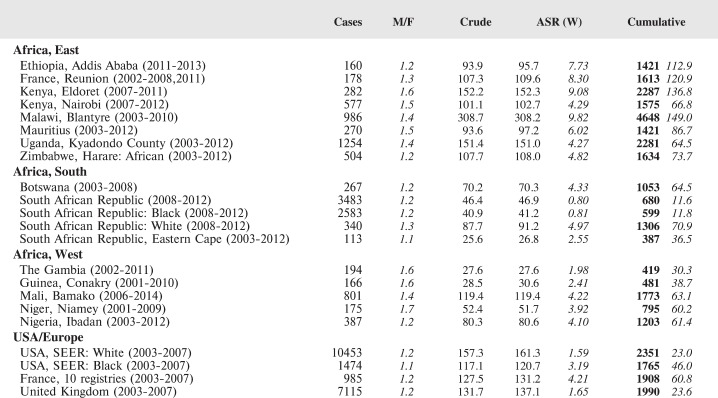
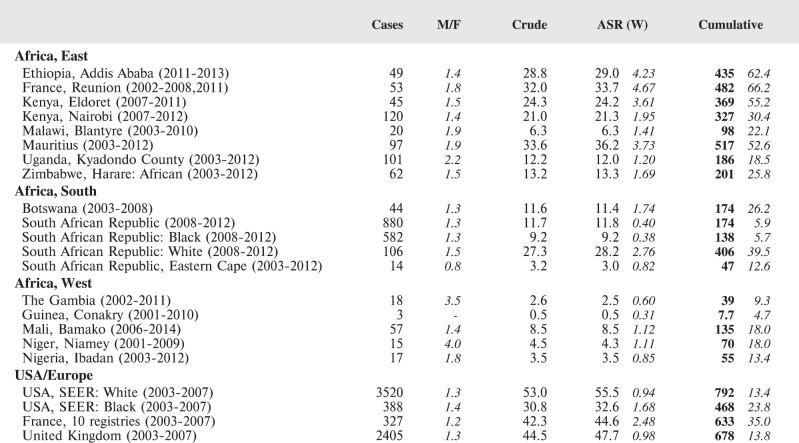
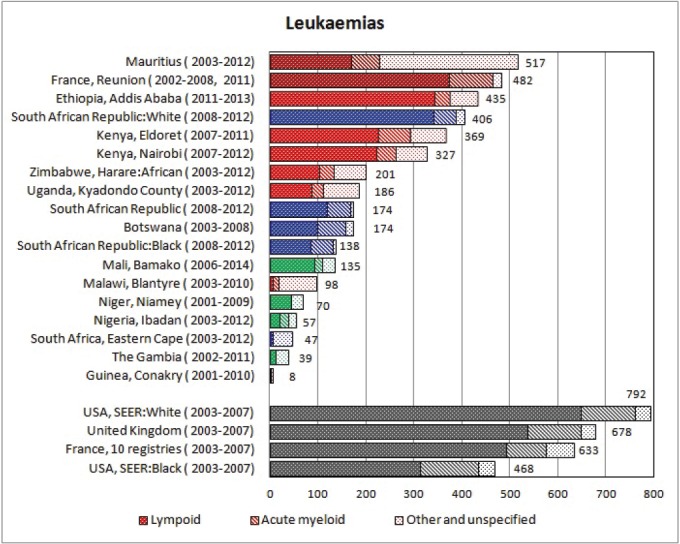
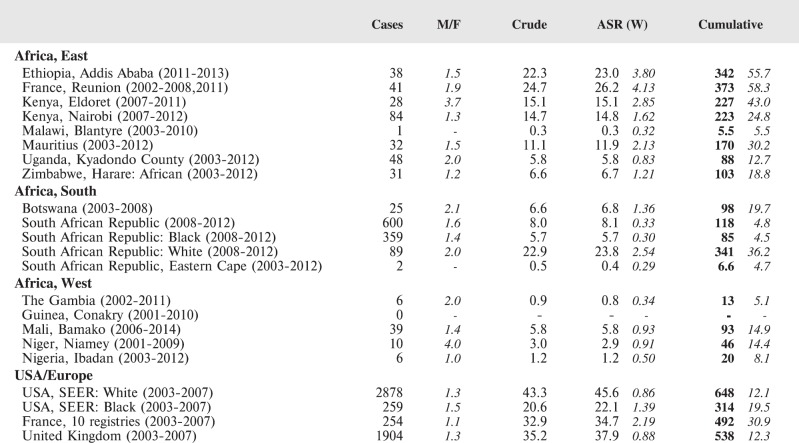
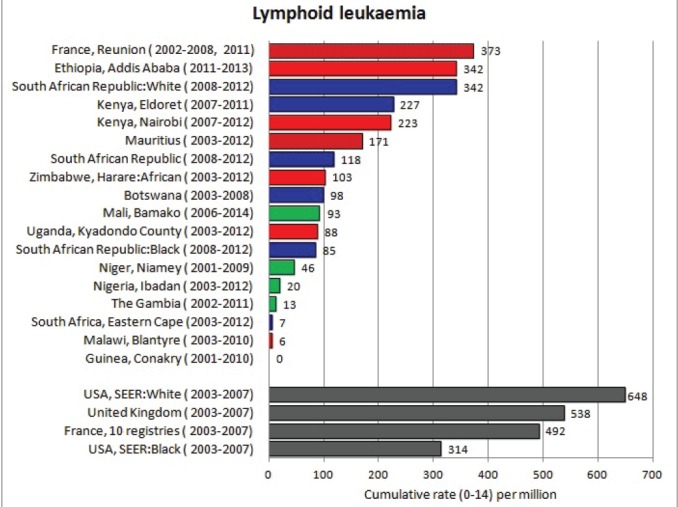
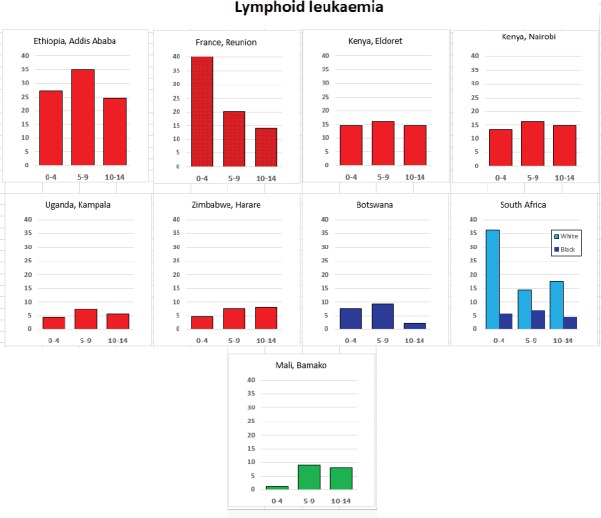
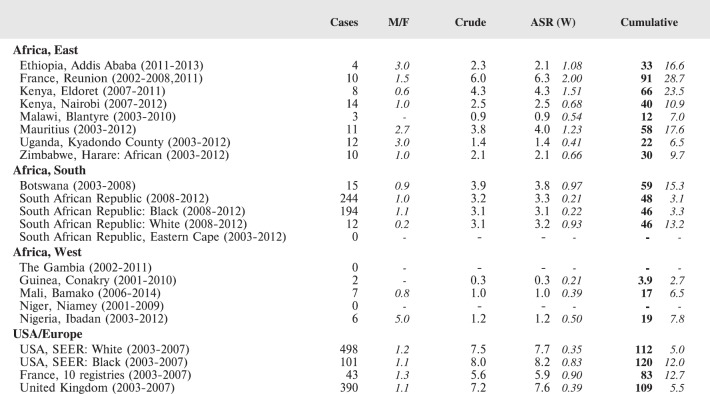
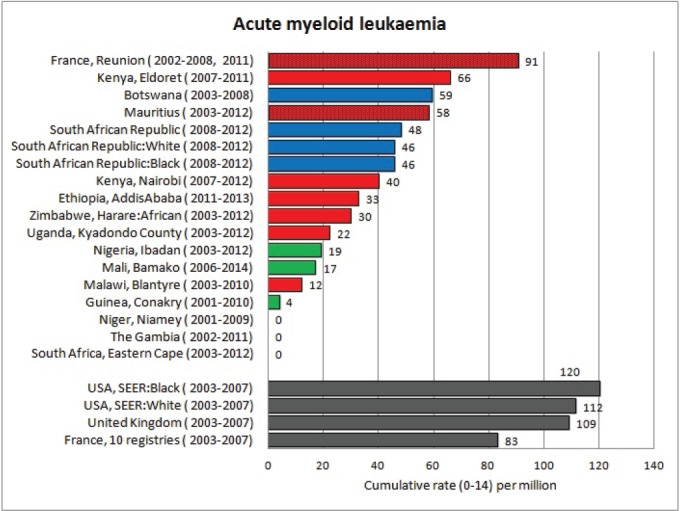
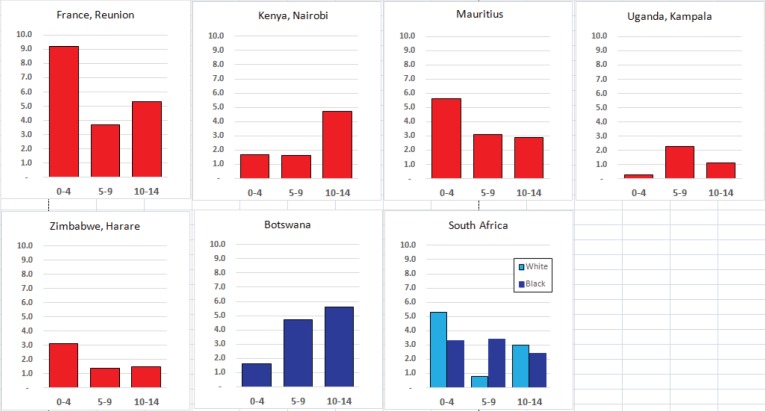
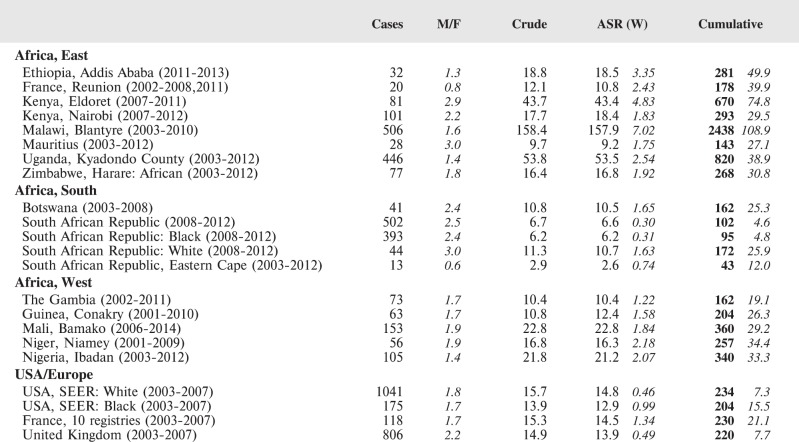
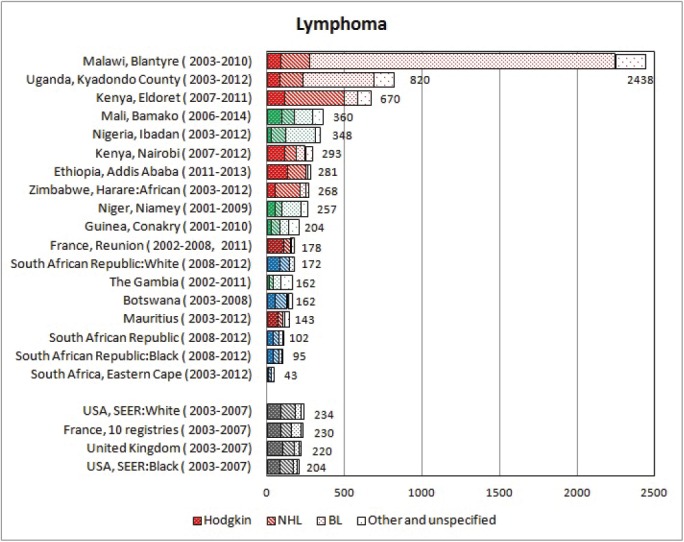
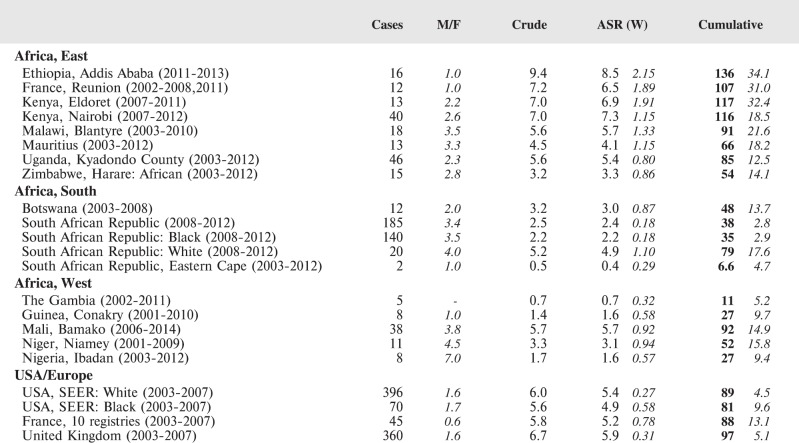
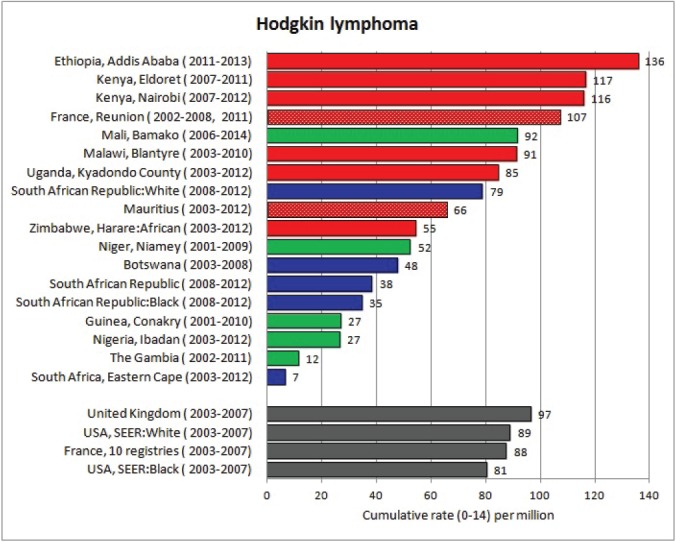
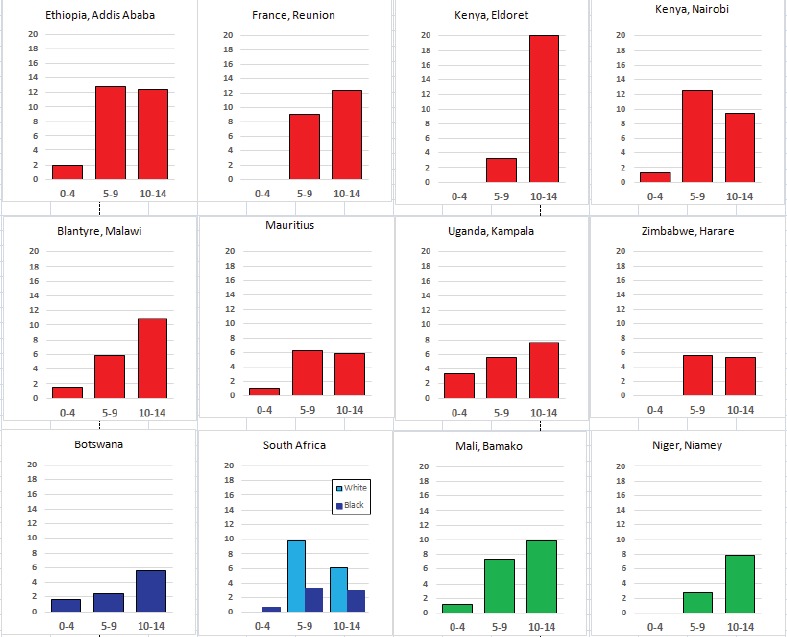
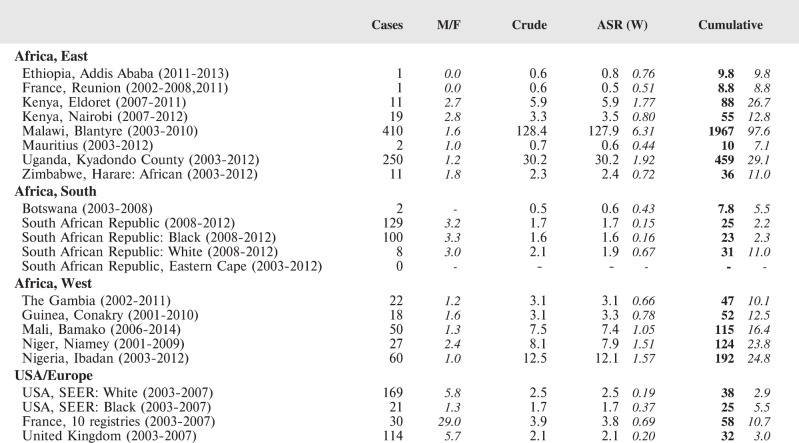
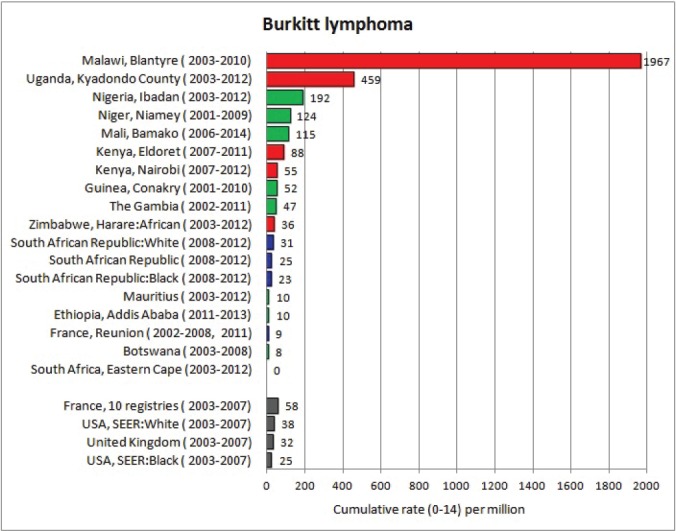
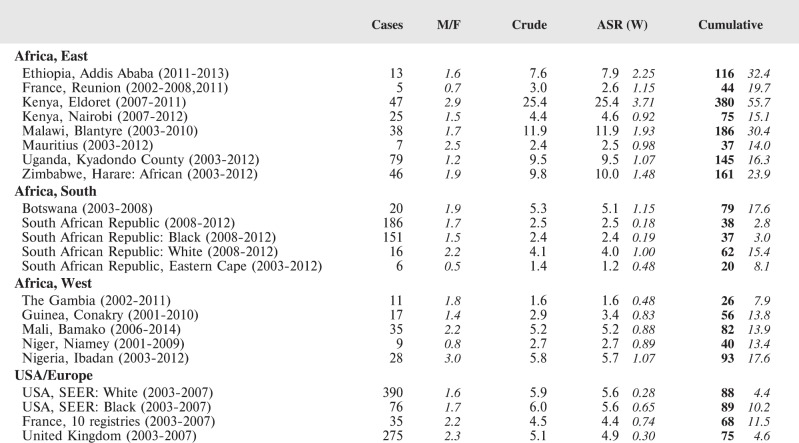
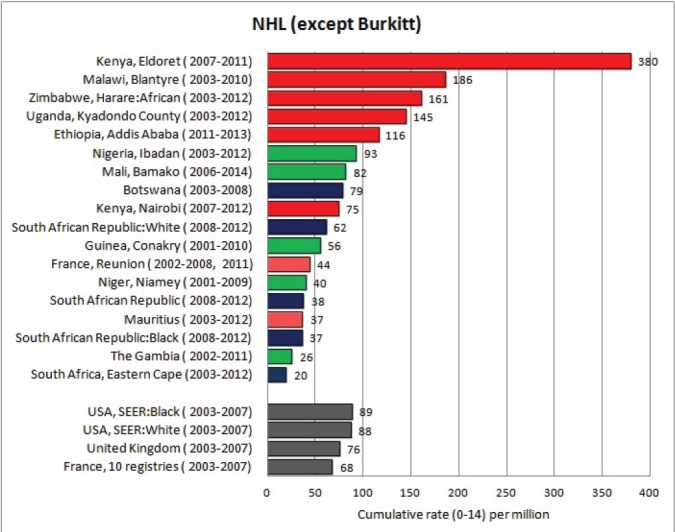
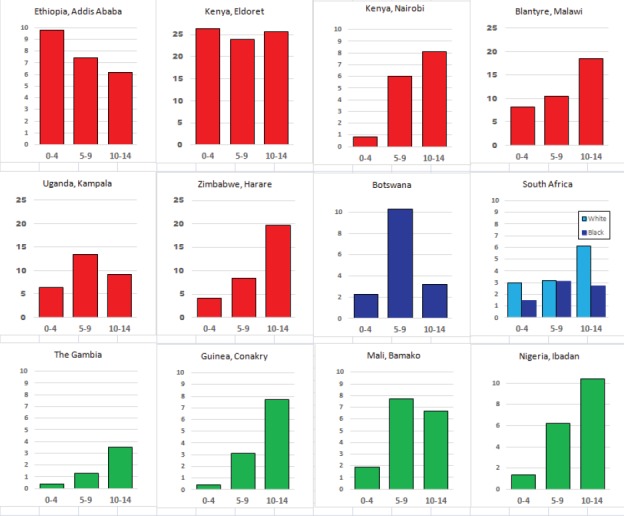
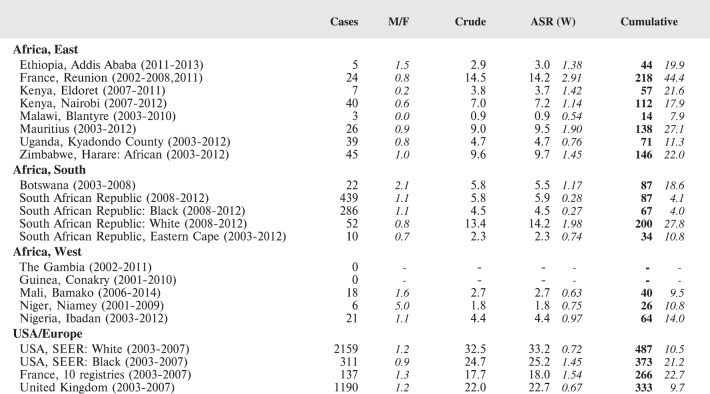
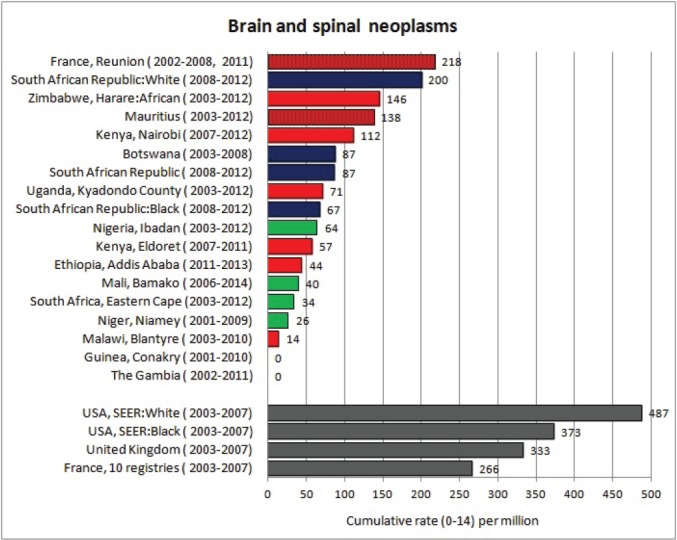
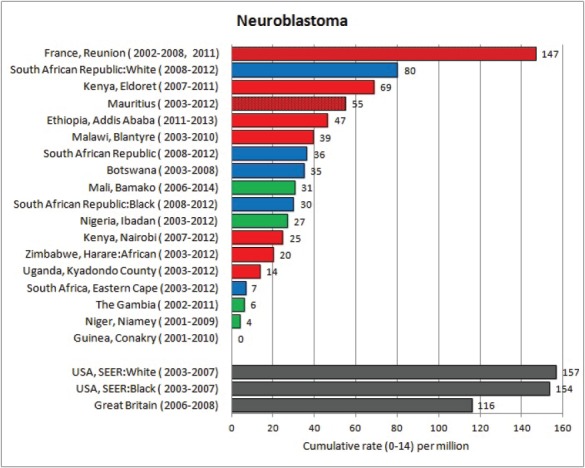
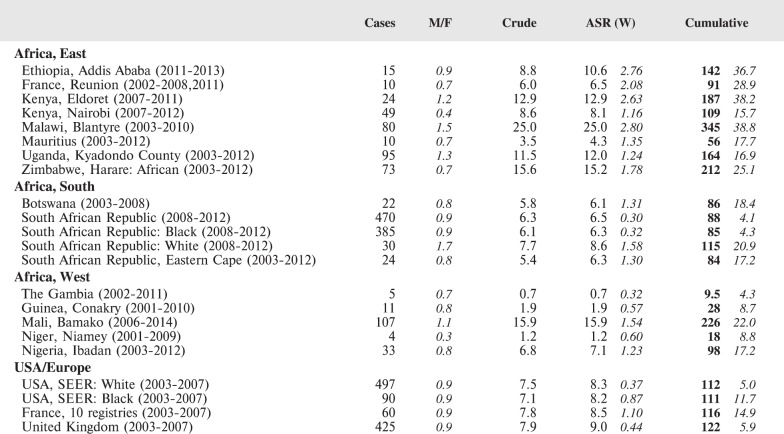
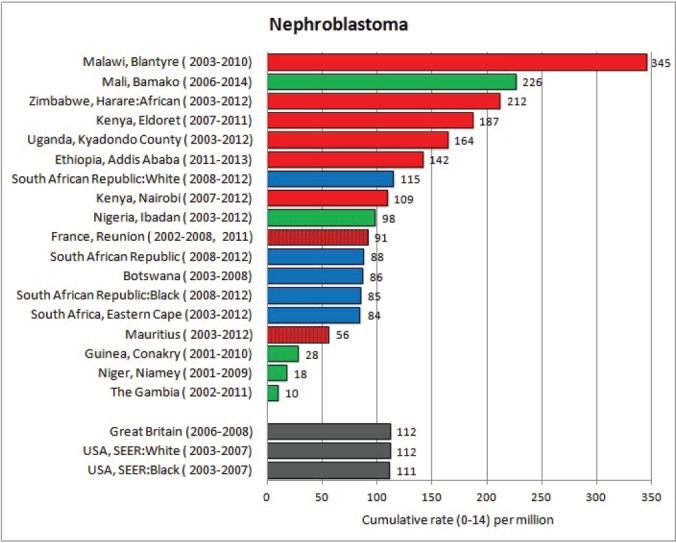
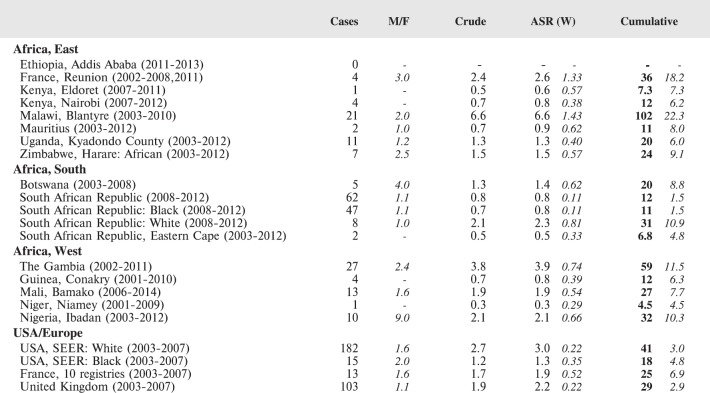
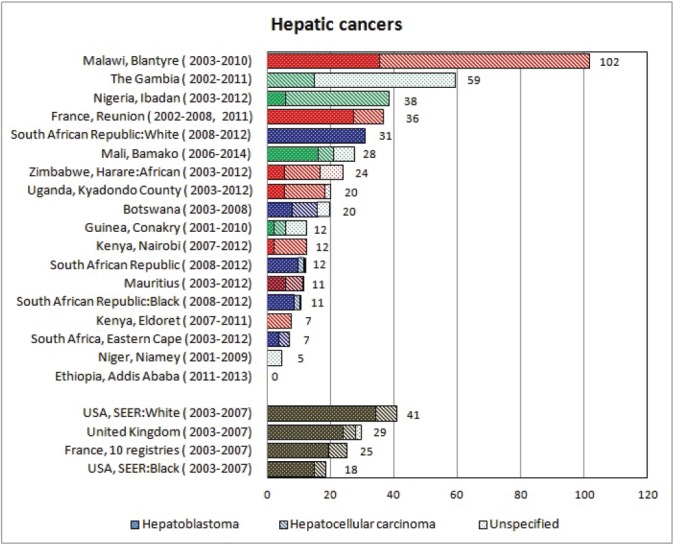
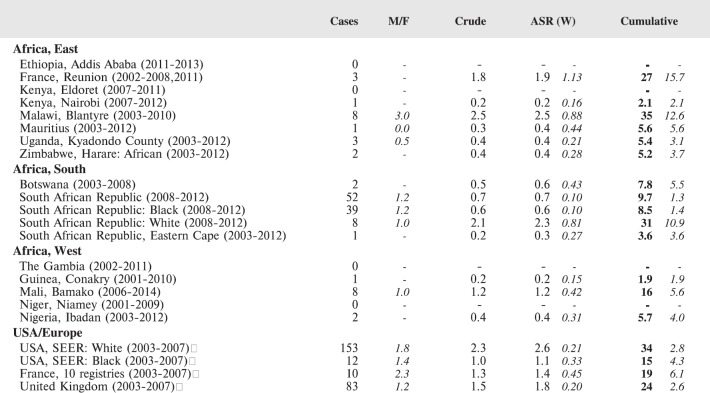
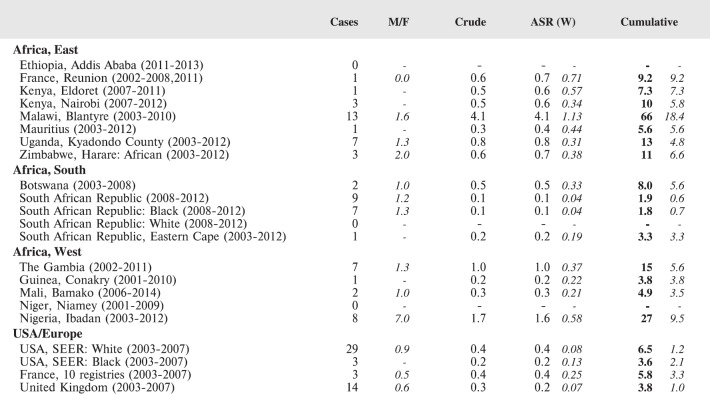
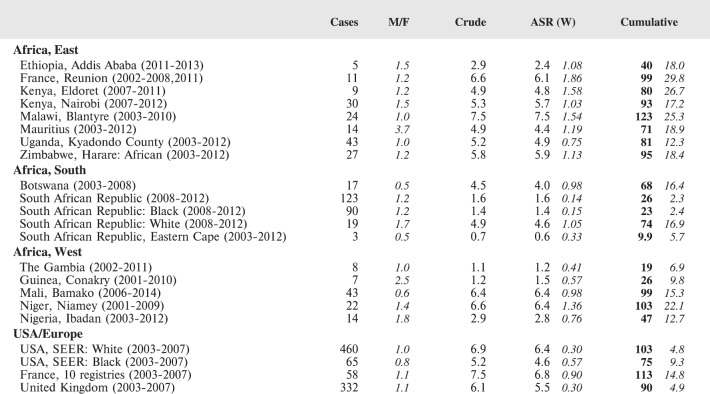
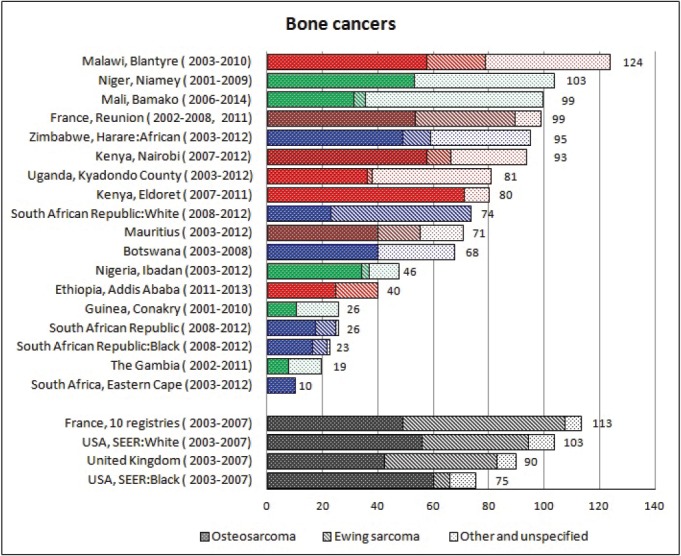
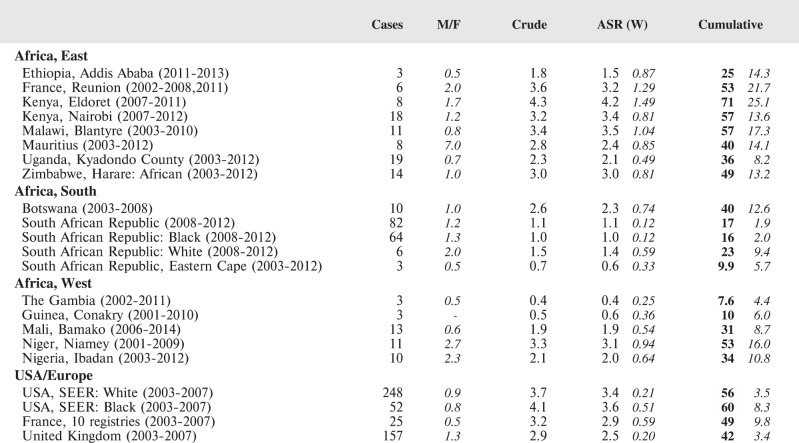
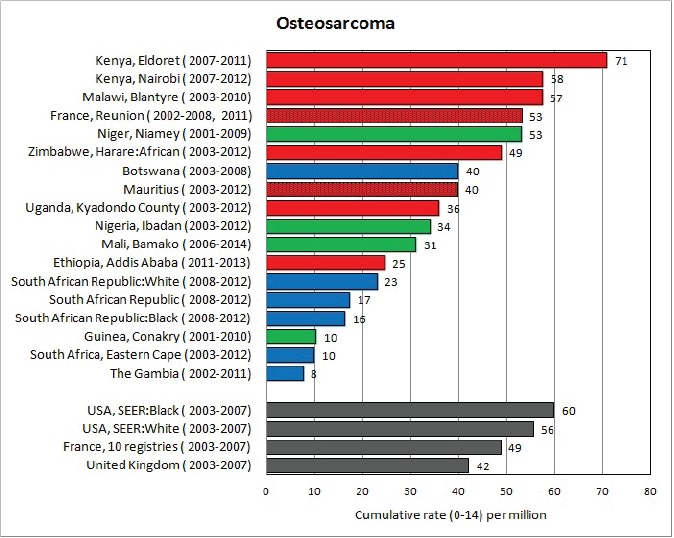
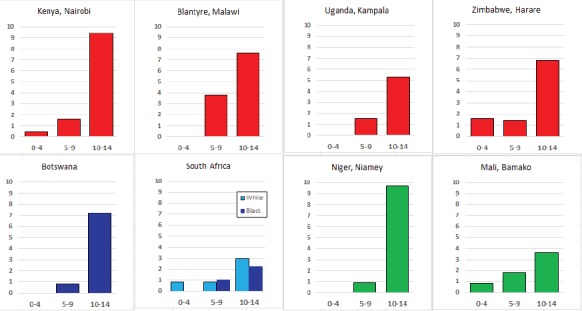
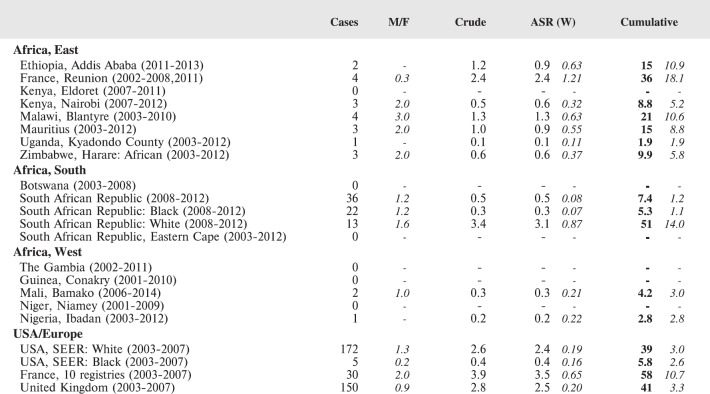
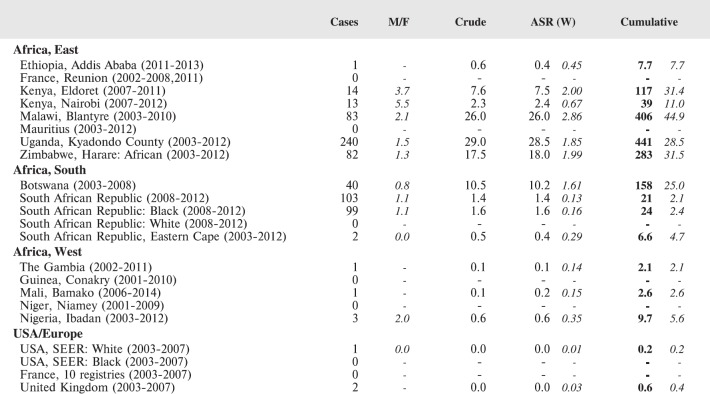
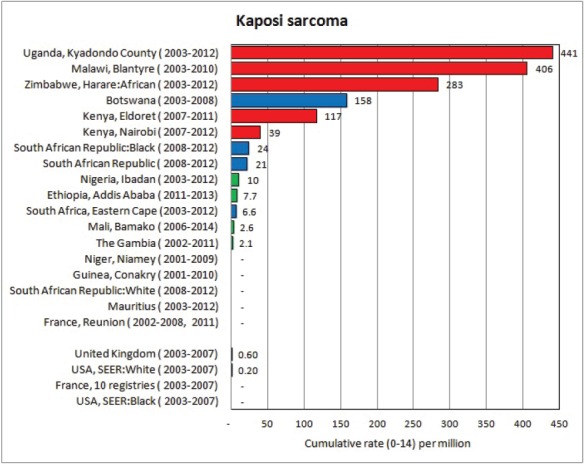
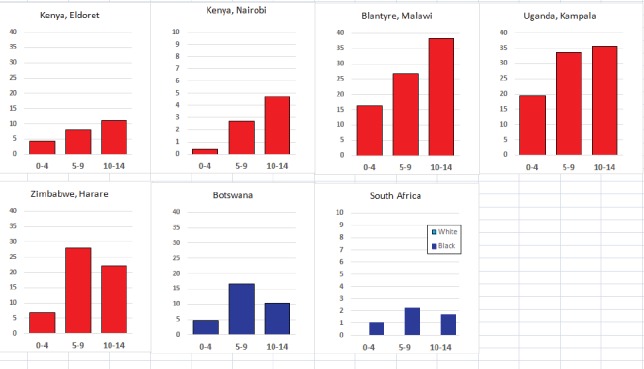
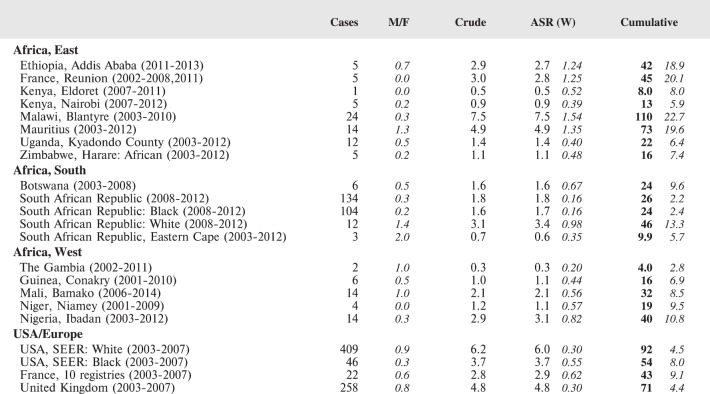
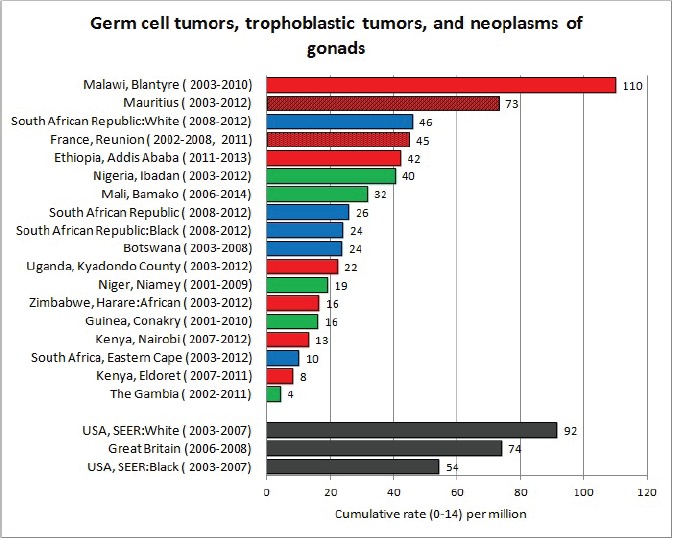
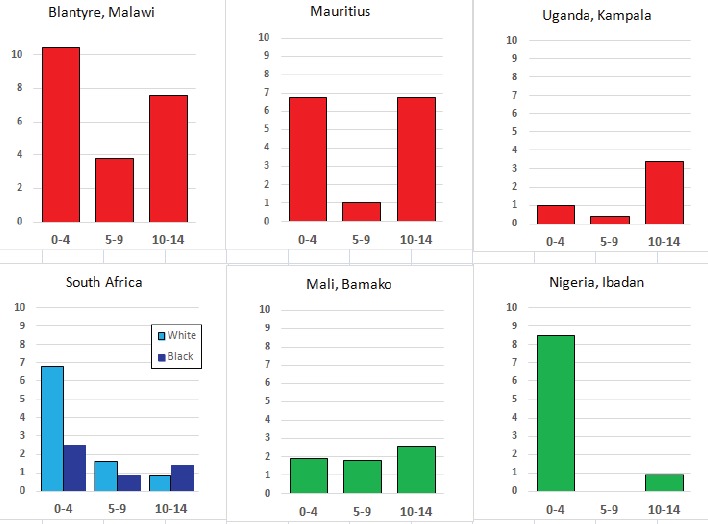
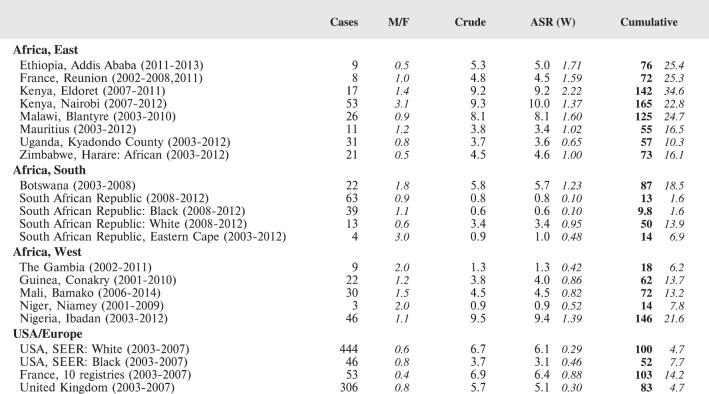
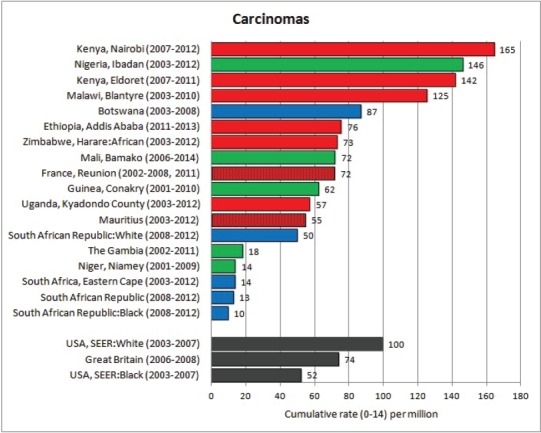
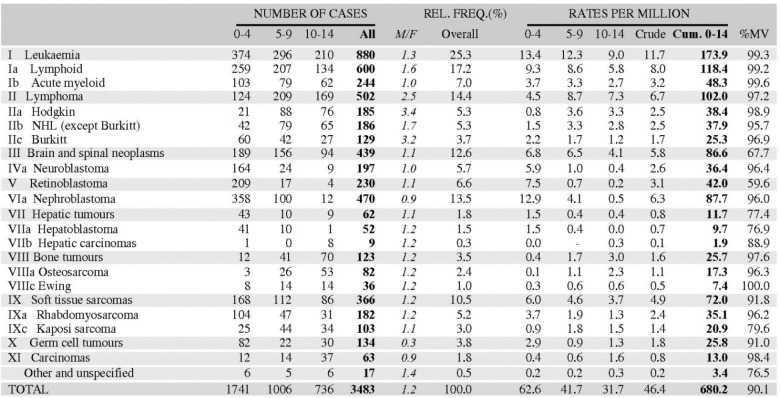
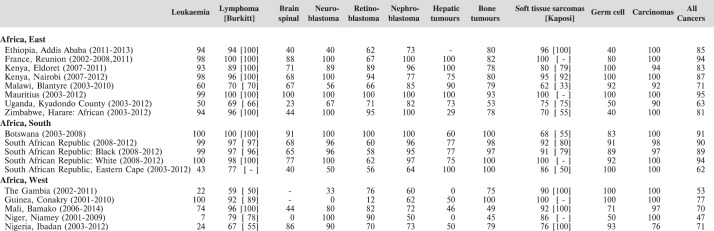
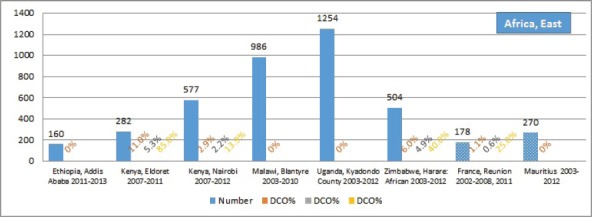
Measurement of incidence rates of childhood cancer in Africa is difficult. The study 'Cancer of Childhood in sub Saharan Africa' brings together results from 16 population-based registries which, as members of the African Cancer Registry Network (AFCRN), have been evaluated as achieving adequate coverage of their target population. The cancers are classified according to the third revision of the International Classification of Childhood Cancer (ICCC-3) and recorded rates in Africa are compared with those in childhood populations in the UK, France, and the USA. It is clear that, in many centres, lack of adequate diagnostic and treatment facilities leads to under-diagnosis (and enumeration) of leukaemias and brain cancers. However, for several childhood cancers, incidence rates in Africa are higher than those in high-income countries. This applies to infection-related cancers such as Kaposi sarcoma, Burkitt lymphoma, Hodgkin lymphoma and hepatocellular carcinoma, and also to two common embryonal cancers - retinoblastoma and nephroblastoma. These (and other) observations are unlikely to be artefact, and are of considerable interest when considering possible aetiological factors, including ethnic differences in risk (and hence genetic/familial antecedents). The data reported are the most extensive so far available on the incidence of cancer in sub Saharan Africa, and clearly indicate the need for more resources to be devoted to cancer registration, especially in the childhood age range, as part of an overall programme to improve the availability of diagnosis and treatment of this group of cancers, many of which have-potentially-an excellent prognosis.
Keywords: cancer; cancer registry; childhood; incidence; sub-Saharan Africa.
Figures








References
-
- Parkin DM, Kramárová E, Draper GJ, et al. IARC Scientific Publications 144; 1998. International incidence of childhood cancer, vol. II.
-
- Parkin DM FJ, Hamdi-Chérif M, Sitas F, et al. IARC Scientific Publications 153; 2003. Cancer in Africa: epidemiology and prevention; pp. 1–414. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources