

Predictive and prognostic impact of tumour-infiltrating lymphocytes in triple-negative breast cancer treated with neoadjuvant chemotherapy
- PMID: 28900472
- PMCID: PMC5574654
- DOI: 10.3332/ecancer.2017.759
Predictive and prognostic impact of tumour-infiltrating lymphocytes in triple-negative breast cancer treated with neoadjuvant chemotherapy
Abstract
Introduction: In locally and locally advanced triple-negative breast cancer (TNBC), neoadjuvant chemotherapy (NAC) only induces a pCR in 30-35% of patients. Clinical and pathological factors are not enough to distinguish the patients who have no chance of a pCR or not. The tumour microenvironment is critical for cancer and tumour-infiltrating lymphocytes (TIL). Moreover, the NAC scenario is the perfect setting to study possible changes in TIL levels.
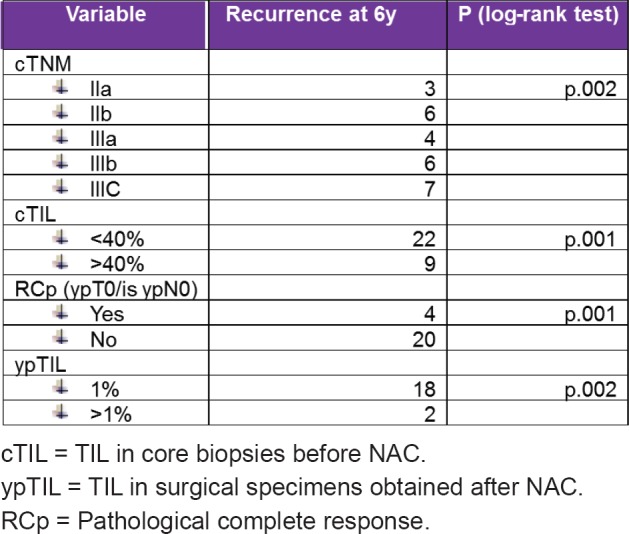
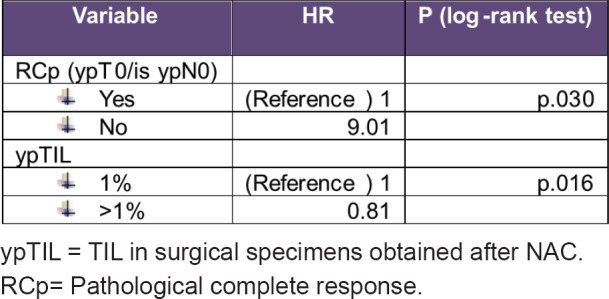
Material and methods: Using our prospective maintained breast cancer (BC) database, we identified 164 TNBC patients treated with NAC between 1998 and 2015 with enough samples of diagnostic biopsy and after surgery. Evaluation of TILs before and after NAC followed a standardised methodology for visual assessment on haematoxylin-eosin sections and the amounts of TILs were quantitated in deciles. We categorised lymphocyte-predominant breast cancer cutoff according to a receiver operating characteristic (ROC) analysis. We categorised LPBC as involving > 40% lymphocytic infiltration tumour stroma. The primary end point was predictive value of TILs to NAC, and the secondary end point was disease-free survival (DFS). DFS was analysed using the Kaplan-Meier method and the groups were compared with a long-rank test. Univariate and multivariate Cox models were used to generate hazard ratios for determining associations between variables such as TIL after NAC and DFS.
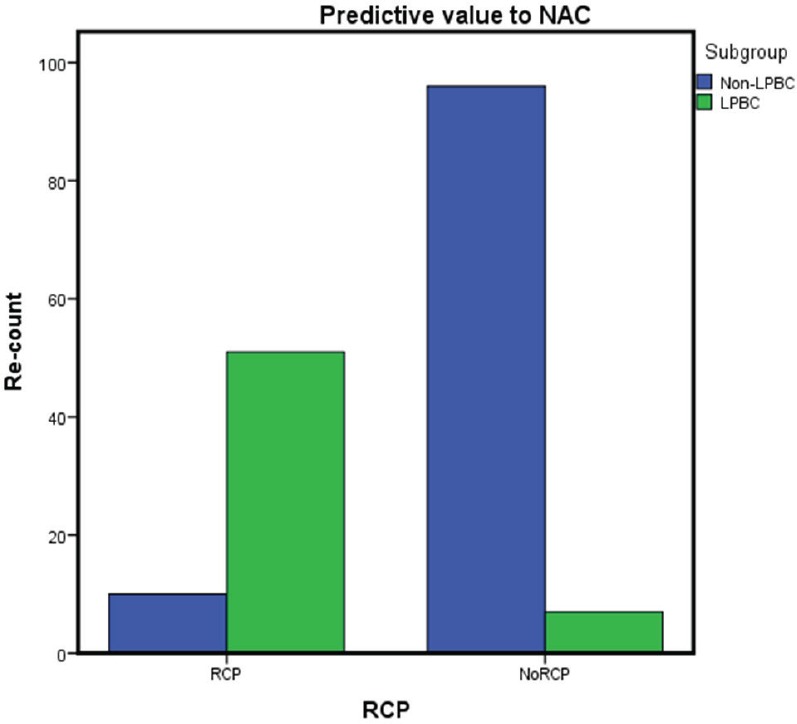
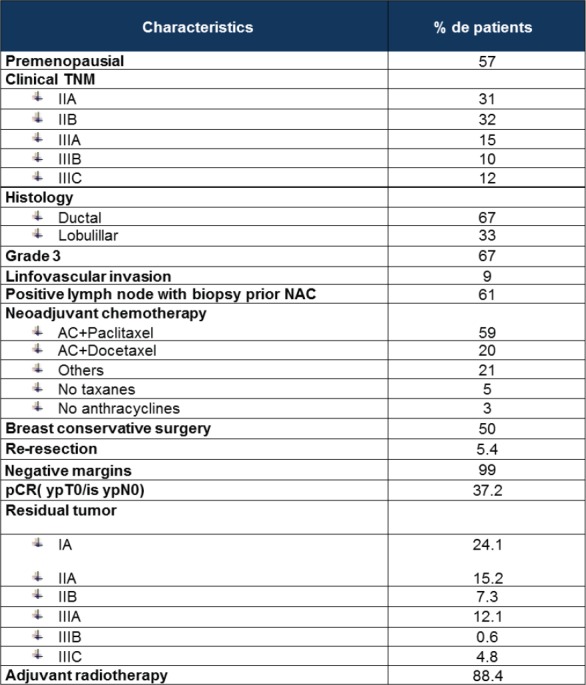
Results: A total of 164 TNBC patients were treated with NAC and surgery. The main patients' characteristics are listed in Table 1. We identify different pathological complete response to anthracycline and taxane-based NAC; LPBC subgroup 51 from 58 patients (88%) pCR versus non- lymphocyte-predominant breast cancer (LPBC) subgroup 10 from 106 (9%) pCR, p = 0.001. At a median follow-up of 78 months, LPBC was associated with better DFS; the three-year Kaplan-Meier estimates for DFS were 2% and 30 % for patients with LPBC and non-LPBC, respectively, p = 0.01. Univariate and multivariate analysis confirmed TIL to be an independent prognostic marker of DFS.
Conclusions: Tumour-infiltrating lymphocytes could be routinely used in locally advanced TNBC treated with anthracycline and taxane, such as biomarker, to be enabled the identification of different two subgroups: LPBC patients have a very high response to NAC pCR 88%, meanwhile non-LPBC patients only achieve 9%. Moreover, non-LPBC patients have a worse prognosis than LPBC patients. This data verified the predictive and prognostic value of TIL.
Keywords: predictive; prognostic value; triple-negative breast cancer; tumour-infiltrating lymphocytes.
Figures

References
-
- Balko JM, Giltnane JM, Wang K, et al. Molecular profiling of the residual disease of triple-negative breast cancers after neoadjuvant chemotherapy identifies actionable therapeutic targets. Cancer Discov. 2014;4(2):223–245. doi: 10.1158/2159-8290.CD-13-0286. - DOI - PMC - PubMed
-
- Loi S, Sirtaine N, Piette F, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol. 2013;31(7):860–867. doi: 10.1200/JCO.2011.41.0902. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources