

Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009-2014
- PMID: 28903154
- PMCID: PMC5710396
- DOI: 10.1001/jama.2017.13836
Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009-2014
Abstract
Importance: Estimates from claims-based analyses suggest that the incidence of sepsis is increasing and mortality rates from sepsis are decreasing. However, estimates from claims data may lack clinical fidelity and can be affected by changing diagnosis and coding practices over time.
Objective: To estimate the US national incidence of sepsis and trends using detailed clinical data from the electronic health record (EHR) systems of diverse hospitals.
Design, setting, and population: Retrospective cohort study of adult patients admitted to 409 academic, community, and federal hospitals from 2009-2014.
Exposures: Sepsis was identified using clinical indicators of presumed infection and concurrent acute organ dysfunction, adapting Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) criteria for objective and consistent EHR-based surveillance.
Main outcomes and measures: Sepsis incidence, outcomes, and trends from 2009-2014 were calculated using regression models and compared with claims-based estimates using International Classification of Diseases, Ninth Revision, Clinical Modification codes for severe sepsis or septic shock. Case-finding criteria were validated against Sepsis-3 criteria using medical record reviews.
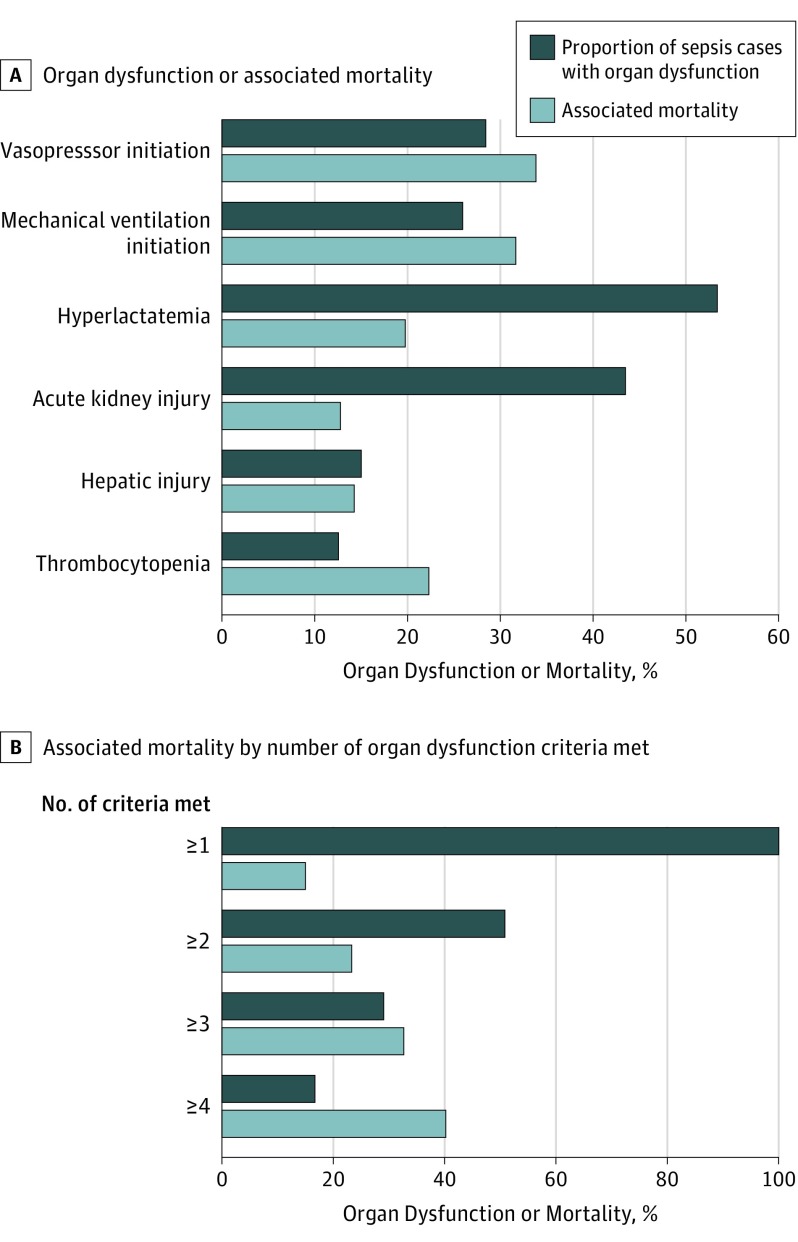
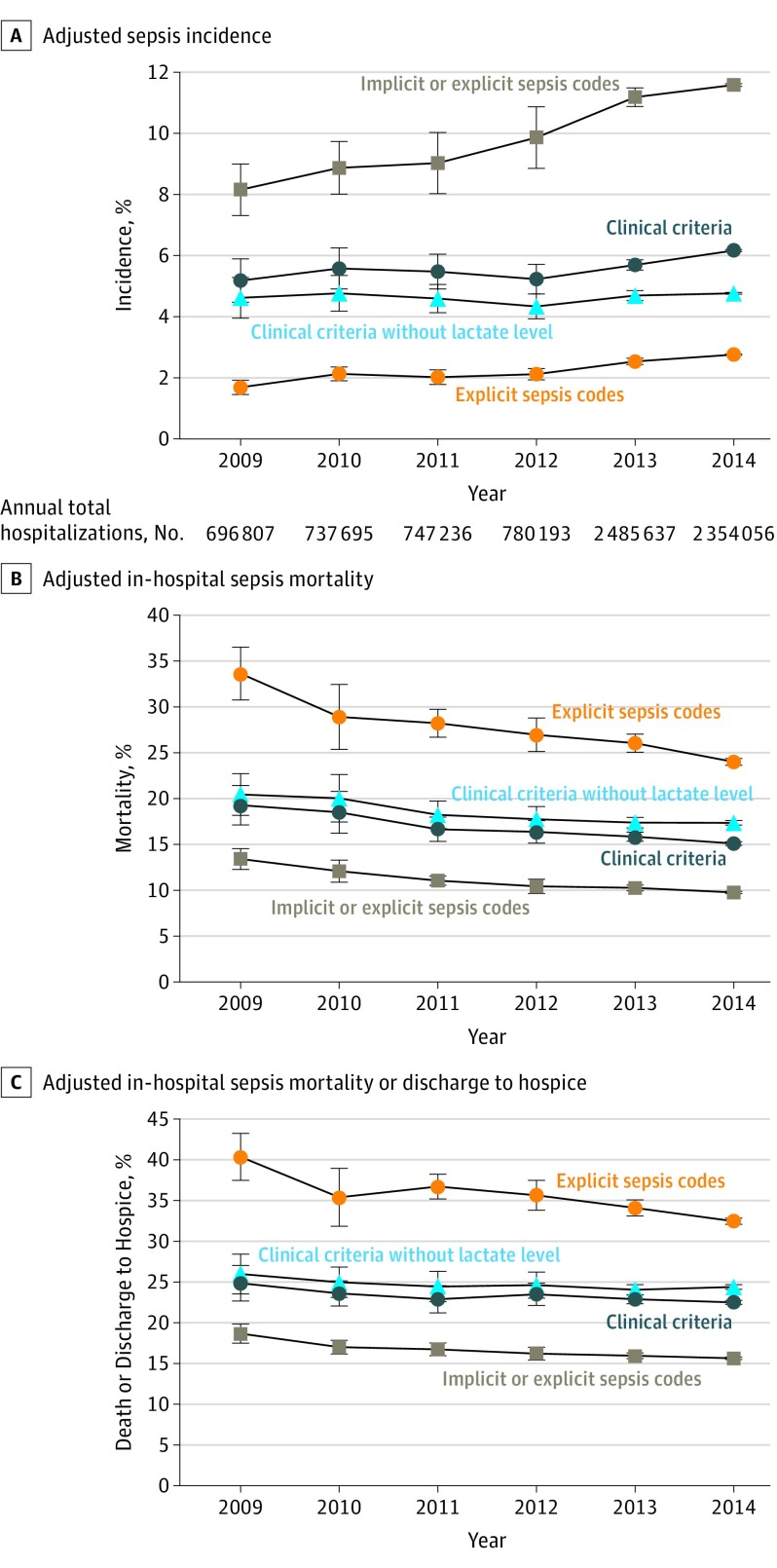
Results: A total of 173 690 sepsis cases (mean age, 66.5 [SD, 15.5] y; 77 660 [42.4%] women) were identified using clinical criteria among 2 901 019 adults admitted to study hospitals in 2014 (6.0% incidence). Of these, 26 061 (15.0%) died in the hospital and 10 731 (6.2%) were discharged to hospice. From 2009-2014, sepsis incidence using clinical criteria was stable (+0.6% relative change/y [95% CI, -2.3% to 3.5%], P = .67) whereas incidence per claims increased (+10.3%/y [95% CI, 7.2% to 13.3%], P < .001). In-hospital mortality using clinical criteria declined (-3.3%/y [95% CI, -5.6% to -1.0%], P = .004), but there was no significant change in the combined outcome of death or discharge to hospice (-1.3%/y [95% CI, -3.2% to 0.6%], P = .19). In contrast, mortality using claims declined significantly (-7.0%/y [95% CI, -8.8% to -5.2%], P < .001), as did death or discharge to hospice (-4.5%/y [95% CI, -6.1% to -2.8%], P < .001). Clinical criteria were more sensitive in identifying sepsis than claims (69.7% [95% CI, 52.9% to 92.0%] vs 32.3% [95% CI, 24.4% to 43.0%], P < .001), with comparable positive predictive value (70.4% [95% CI, 64.0% to 76.8%] vs 75.2% [95% CI, 69.8% to 80.6%], P = .23).
Conclusions and relevance: In clinical data from 409 hospitals, sepsis was present in 6% of adult hospitalizations, and in contrast to claims-based analyses, neither the incidence of sepsis nor the combined outcome of death or discharge to hospice changed significantly between 2009-2014. The findings also suggest that EHR-based clinical data provide more objective estimates than claims-based data for sepsis surveillance.
Conflict of interest statement
Figures
Comment in
-
Counting Sepsis, an Imprecise but Improving Science.JAMA. 2017 Oct 3;318(13):1228-1229. doi: 10.1001/jama.2017.13697. JAMA. 2017. PMID: 28903164 No abstract available.
References
-
- Torio CM, Andrews RM National inpatient hospital costs: the most expensive conditions by payer, 2011: Statistical Brief 160. Healthcare Cost and Utilization Project (HCUP) website. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb160.jsp. 2006. Accessed August 31, 2017. - PubMed
-
- Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90-92. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546-1554. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007;35(5):1244-1250. - PubMed
-
- Lagu T, Rothberg MB, Shieh MS, Pekow PS, Steingrub JS, Lindenauer PK. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40(3):754-761. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
