

Locoregionally recurrent head and neck squamous cell carcinoma: incidence, survival, prognostic factors, and treatment outcomes
- PMID: 28903447
- PMCID: PMC5589686
- DOI: 10.18632/oncotarget.16340
Locoregionally recurrent head and neck squamous cell carcinoma: incidence, survival, prognostic factors, and treatment outcomes
Abstract
Purpose: For locoregionally recurrent head and neck squamous cell carcinoma (HNSCC), appropriate therapeutic decisions remain unclear. We examined the treatment outcomes of a national cohort to determine suitable treatments for and prognostic factors in patients with locoregionally recurrent HNSCCs at different stages and sites.
Patients and methods: We analyzed data of >20-year-old patients with HNSCC at American Joint Committee on Cancer clinical stages I-IV without metastasis from Taiwan National Health Insurance and cancer registry databases. The index date was the date of recurrent HNSCC diagnosis. Recurrent HNSCC was defined as the annotation of locoregional recurrence with tissue proof in cancer registry databases. The enrolled patients were categorized into three groups: Group 1 comprised those undergoing chemotherapy (CT) alone; Group 2 comprised those receiving reirradiation (re-RT) alone (total radiation dose ≥ 60 Gy through intensity modulation radiation therapy [IMRT]); Group 3 comprised those receiving concurrent chemoradiotherapy (CCRT) alone (irradiation total dose ≥60 Gy through IMRT); and Group 4 comprised those receiving salvage surgery with or without RT or CT.
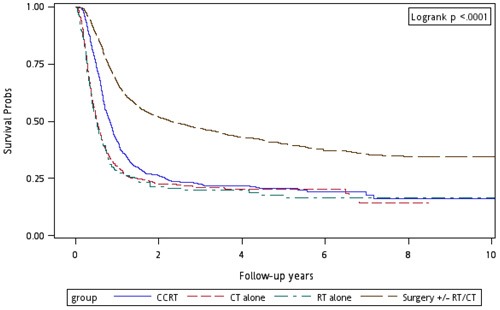
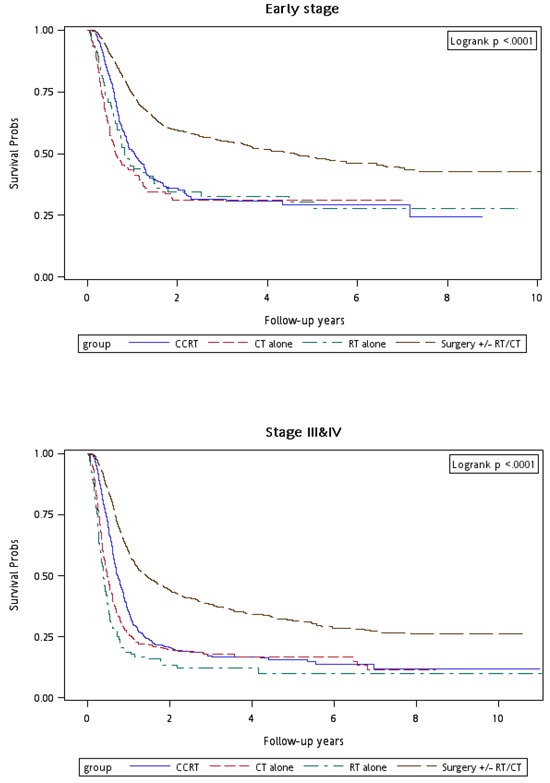
Results: We enrolled 4,839 and 28,664 HNSCC patients with and without locoregional recurrence, respectively (median follow-up, 3.25 years). Locoregional recurrence rate and incidence were 14.44% and 40.73 per 1,000 person-years, respectively. Age ≥ 65 years, Charlson comorbidity index (CCI) score > 6, advanced clinical stage at first diagnosis, and recurrence-free interval < 1 year were significant independent prognostic risk factors for overall survival as per univariate and multivariate Cox regression analyses. After adjusting for age, sex, CCI scores, clinical stage at first diagnosis, and recurrence-free interval, adjusted hazard ratios (aHRs; 95% confidence intervals [CIs]) for overall mortality in recurrent clinical stages I and II were 0.63 (0.45-0.89, p = 0.009), 0.65 (0.52-0.83, p < 0.001), and 0.32 (0.26-0.40, p < 0.001) in Groups 2, 3, and 4, respectively, whereas they were 1.23 (0.99-1.52, p = 0.062), 0.69 (0.60-0.79, p < 0.001), and 0.39 (0.34-0.44, p < 0.001) for Groups 2, 3, and 4, respectively, for overall mortality in recurrent clinical stage III and IV.
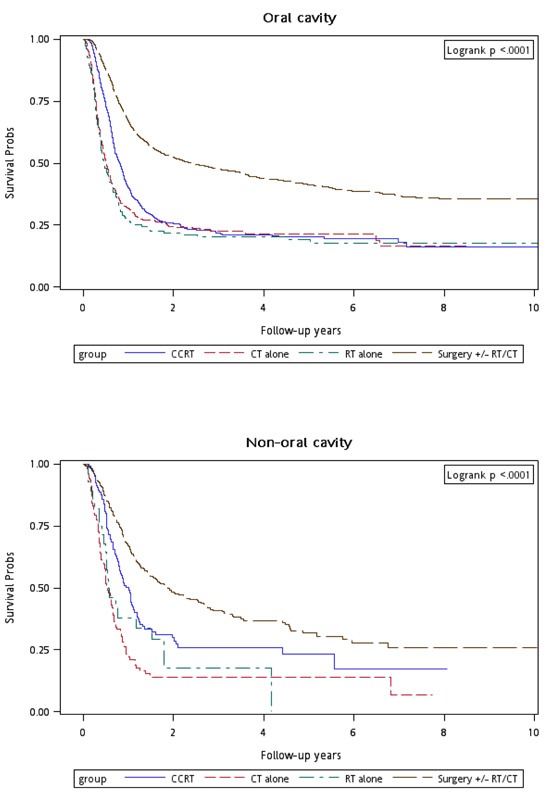
Conclusions: Age, CCI score, clinical stage at first diagnosis, and recurrence-free interval are significant independent prognostic factors for overall survival of recurrent HNSCC patients. Regardless of recurrence stage or site, salvage surgery is the recommended first recurrent HNSCC treatment choice. Re-RT alone and CCRT are more suitable for inoperable recurrent early-stage oral and nonoral cavity recurrent HNSCCs, respectively.
Keywords: head and neck cancer; incidence; prognostic factors; recurrence; survival.
Conflict of interest statement
CONFLICTS OF INTEREST The author(s) indicate that no potential conflicts of interest exist. Employment or Leadership Position: None Consultant or Advisory Role: None Stock Ownership: None Honoraria: None Research Funding: Wang Fang Hospital funding: 106-swf-08 Expert Testimony: None Patents: None Other Remuneration: None
Figures
References
-
- Janot F, de Raucourt D, Benhamou E, Ferron C, Dolivet G, Bensadoun RJ, Hamoir M, Géry B, Julieron M, Castaing M, Bardet E, Grégoire V, Bourhis J. Randomized trial of postoperative reirradiation combined with chemotherapy after salvage surgery compared with salvage surgery alone in head and neck carcinoma. J Clin Oncol. 2008;26:5518–23. - PubMed
-
- Salama JK, Vokes EE. Concurrent chemotherapy and re-irradiation for locoregionally recurrent head and neck cancer. Semin Oncol. 2008;35:251–61. - PubMed
-
- Lee N, Chan K, Bekelman JE, Zhung J, Mechalakos J, Narayana A, Wolden S, Venkatraman ES, Pfister D, Kraus D, Shah J, Zelefsky MJ. Salvage re-irradiation for recurrent head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;68:731–40. - PubMed
-
- Goodwin WJ., Jr Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: when do the ends justify the means? Laryngoscope. 2000;110(Suppl 93):1–18. - PubMed
-
- Posner MR, Hershock DM, Blajman CR, Mickiewicz E, Winquist E, Gorbounova V, Tjulandin S, Shin DM, Cullen K, Ervin TJ, Murphy BA, Raez LE, Cohen RB, et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med. 2007;357:1705–15. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
