

Biosimilars in rheumatology: A review of the evidence and their place in the treatment algorithm
- PMID: 28903543
- PMCID: PMC5850807
- DOI: 10.1093/rheumatology/kex277
Biosimilars in rheumatology: A review of the evidence and their place in the treatment algorithm
Abstract
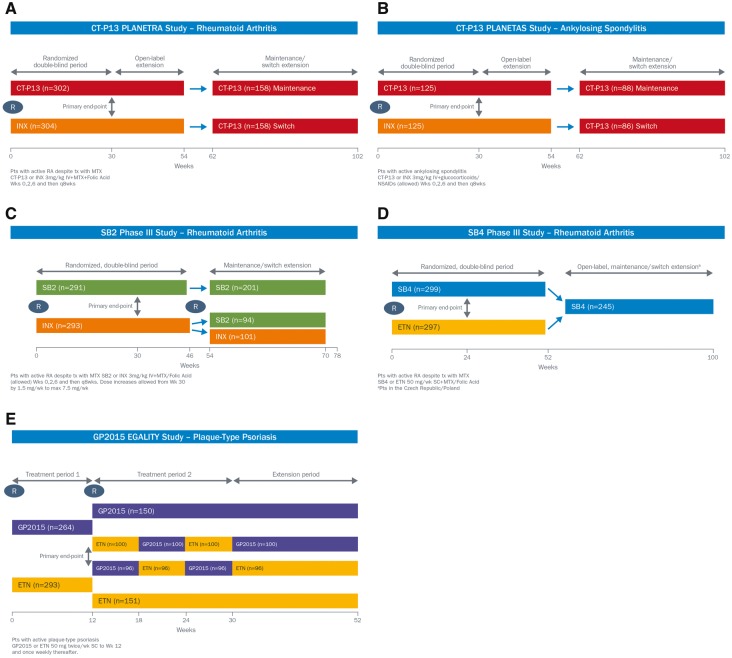
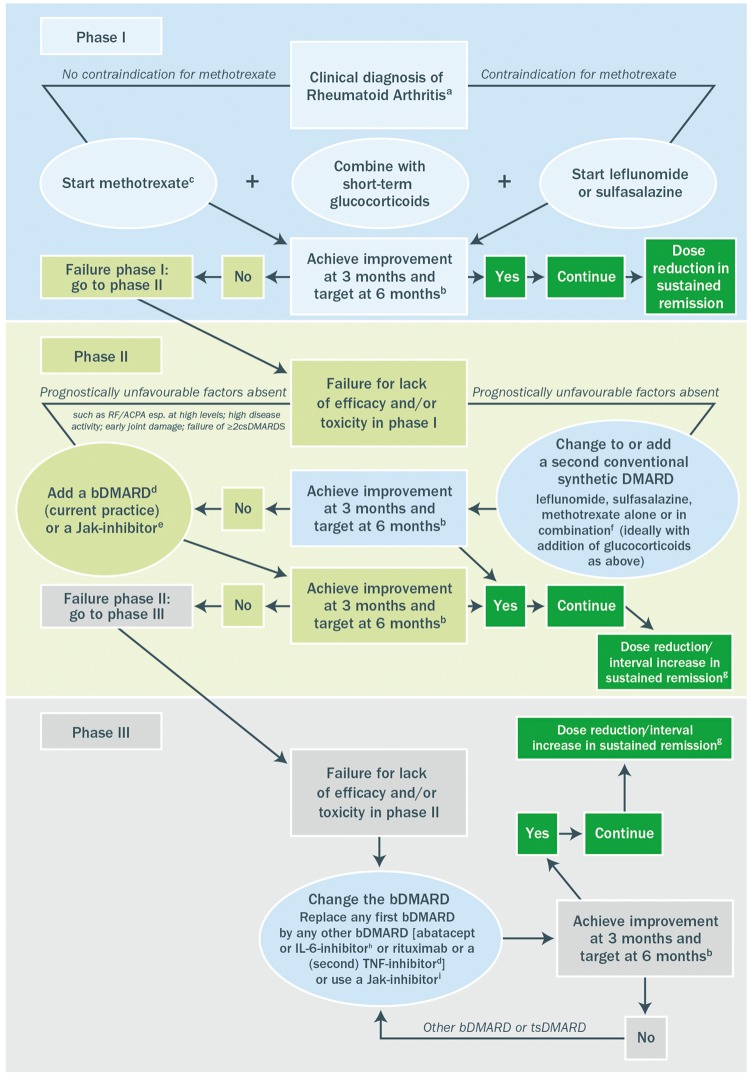
Determining biosimilarity involves a comprehensive exercise with a focus on determining the comparability of the molecular characteristics and preclinical profile of the biosimilar and reference product, such that there is less need for extensive clinical testing to assure comparability of clinical outcomes. Three anti-TNF biosimilar agents are approved for patients with rheumatic diseases in the European Union. The infliximab (Remicade®) biosimilars CT-P13 (Remsima® and Inflectra®) and SB2 (Flixabi®) and the etanercept (Enbrel®) biosimilar SB4 (Benepali®) have shown close comparability to their reference medicinal products, having undergone extensive evaluations. Guidelines on the treatment of rheumatic diseases have acknowledged that biosimilars and biologic DMARDs (bDMARDs) are interchangeable in clinical practice, except when patients experience lack of efficacy or tolerability with the reference agent. Given that cost is a barrier to effective bDMARD use, the introduction of less costly biosimilars is likely to widen access and dissipate treatment inequalities. Physicians faced with prescribing decisions should be reassured by the robust and exhaustive process that is involved in assuring comparability of biosimilars with their reference agents. De novo usage of a biosimilar and switching to a biosimilar following lack of efficacy or tolerability with a different reference biologic agent are likely to be strategies most easily adopted, although switching during successful treatment should also be considered given the potential cost implications. The introduction of biosimilar bDMARDs has the potential to improve patient access to effective biologic therapy, to better accommodate restraints within healthcare budgets and to improve overall patient outcomes.
Keywords: CT-P13; SB2; SB4; biosimilar; rheumatic disease.
© The Author 2017. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
References
-
- Gartlehner G, Hansen RA, Jonas BL, Thieda P, Lohr KN.. The comparative efficacy and safety of biologics for the treatment of rheumatoid arthritis: a systematic review and meta-analysis. J Rheumatol 2006;33:30–48. - PubMed
-
- Coates LC, Tillett W, Chandler D. et al. The 2012 BSR and BHPR guideline for the treatment of psoriatic arthritis with biologics. Rheumatology 2013;52:1754–7. - PubMed
-
- Smith CH, Astey AS, Barker JN. et al. British Association of Dermatologists’ guidelines for biologic interventions for psoriasis 2009. Br J Dermatol 2009;161:987–1019. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
