

Mesh penetrating the cecum and bladder following inguinal hernia surgery: a case report
- PMID: 28903762
- PMCID: PMC5598008
- DOI: 10.1186/s13256-017-1435-8
Mesh penetrating the cecum and bladder following inguinal hernia surgery: a case report
Abstract
Background: Tension-free repair using mesh is a common inguinal hernia surgical procedure. However, various complications such as mesh-related infection and recurrence may develop as a result. Moreover, although rare, there are also reports of intestinal obstruction caused by adhesion of the mesh to the intestinal wall and cases of mesh migration into various organs. Here, we report our experience with a patient in whom mesh extraction was performed due to migration of mesh into the intestinal tract following inguinal hernia surgery and formation of a fistula with the bladder.
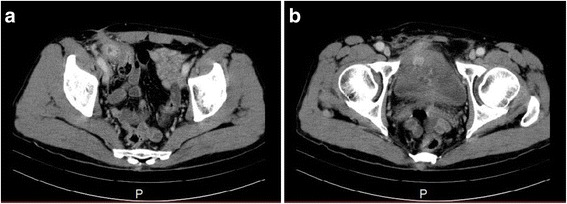
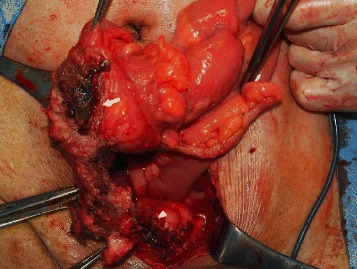
Case presentation: Our patient was a 63-year-old Japanese man who had a history of operative treatment for right inguinal hernia during early childhood. Because a relapse subsequently occurred, he was diagnosed as having recurrent right inguinal hernia at the age of 56 years for which operative treatment (the Kugel method) was performed. He presented to our hospital 6 years later with the chief complaint of lower abdominal pain. Computed tomography findings revealed a mass shadow in contact with his bladder and cecal walls, and enteric bacteria were detected in his urine. Furthermore, because lower gastrointestinal endoscopic findings confirmed mesh in the cecum, we performed operative treatment. The mesh had migrated into the cecum and a fistula with his bladder had formed. We removed the mesh through ileocecal resection and partial cystectomy.
Conclusions: It appeared that a peritoneal defect occurred when the mesh was placed, allowing the mesh to migrate into our patient's intestinal tract. Because contact between the mesh and the cecum resulted in inflammation, a fistula formed in his bladder. It is important to completely close the peritoneum when placing the mesh.
Keywords: Bladder; Cecum; Inguinal hernia; Kugel method; Mesh penetration.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
