

Antiarrhythmic Drugs for Nonshockable-Turned-Shockable Out-of-Hospital Cardiac Arrest: The ALPS Study (Amiodarone, Lidocaine, or Placebo)
- PMID: 28904070
- PMCID: PMC5705566
- DOI: 10.1161/CIRCULATIONAHA.117.028624
Antiarrhythmic Drugs for Nonshockable-Turned-Shockable Out-of-Hospital Cardiac Arrest: The ALPS Study (Amiodarone, Lidocaine, or Placebo)
Abstract
Background: Out-of-hospital cardiac arrest (OHCA) commonly presents with nonshockable rhythms (asystole and pulseless electric activity). It is unknown whether antiarrhythmic drugs are safe and effective when nonshockable rhythms evolve to shockable rhythms (ventricular fibrillation/pulseless ventricular tachycardia [VF/VT]) during resuscitation.
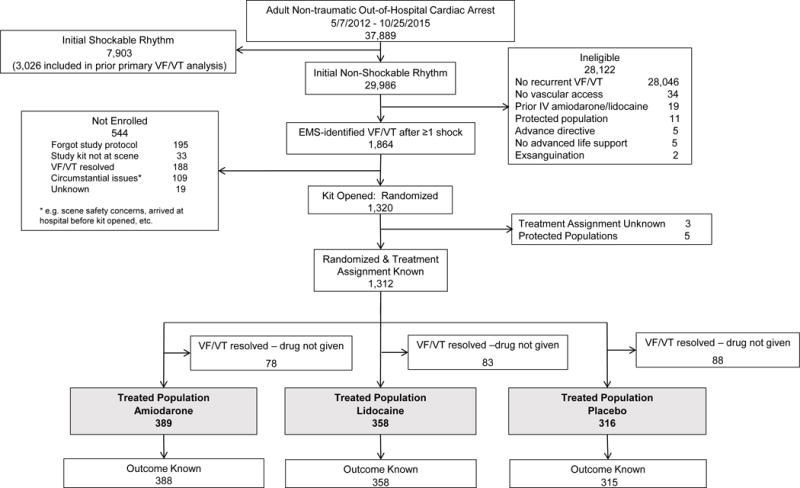
Methods: Adults with nontraumatic OHCA, vascular access, and VF/VT anytime after ≥1 shock(s) were prospectively randomized, double-blind, to receive amiodarone, lidocaine, or placebo by paramedics. Patients presenting with initial shock-refractory VF/VT were previously reported. The current study was a prespecified analysis in a separate cohort that initially presented with nonshockable OHCA and was randomized on subsequently developing shock-refractory VF/VT. The primary outcome was survival to hospital discharge. Secondary outcomes included discharge functional status and adverse drug-related effects.
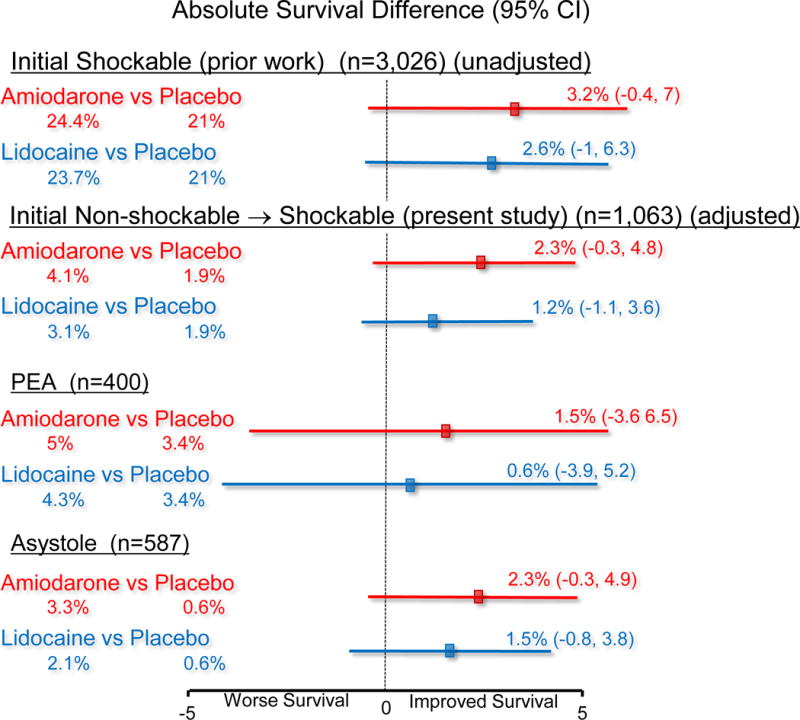
Results: Of 37 889 patients with OHCA, 3026 with initial VF/VT and 1063 with initial nonshockable-turned-shockable rhythms were treatment-eligible, were randomized, and received their assigned drug. Baseline characteristics among patients with nonshockable-turned-shockable rhythms were balanced across treatment arms, except that recipients of a placebo included fewer men and were less likely to receive bystander cardiopulmonary resuscitation. Active-drug recipients in this cohort required fewer shocks, supplemental doses of their assigned drug, and ancillary antiarrhythmic drugs than recipients of a placebo (P<0.05). In all, 16 (4.1%) amiodarone, 11 (3.1%) lidocaine, and 6 (1.9%) placebo-treated patients survived to hospital discharge (P=0.24). No significant interaction between treatment assignment and discharge survival occurred with the initiating OHCA rhythm (asystole, pulseless electric activity, or VF/VT). Survival in each of these categories was consistently higher with active drugs, although the trends were not statistically significant. Adjusted absolute differences (95% confidence interval) in survival from nonshockable-turned-shockable arrhythmias with amiodarone versus placebo were 2.3% (-0.3, 4.8), P=0.08, and for lidocaine versus placebo 1.2% (-1.1, 3.6), P=0.30. More than 50% of these survivors were functionally independent or required minimal assistance. Drug-related adverse effects were infrequent.
Conclusions: Outcome from nonshockable-turned-shockable OHCA is poor but not invariably fatal. Although not statistically significant, point estimates for survival were greater after amiodarone or lidocaine than placebo, without increased risk of adverse effects or disability and consistent with previously observed favorable trends from treatment of initial shock-refractory VF/VT with these drugs. Together the findings may signal a clinical benefit that invites further investigation.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT01401647.
Keywords: amiodarone; cardiac arrest; lidocaine; placebo; resuscitation.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Disclosures
No conflicts of interest relevant to the topic of discussion by any of the authors.
Figures
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozafarrian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritches M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Hu JHY, Alter HM, Wong SS, Muntner P. Heart disease and stroke statistics – 2017 update: A report from the American Heart Association. Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospital cardiac arrest and survival rates. Resuscitation. 2010;81:1479–1487. - PubMed
-
- Cobb LA, Fahrenbruch CE, Olsufka M, Copass MK. Changing incidence of out-of-hospital ventricular fibrillation, 1980–2000. JAMA. 2002;288:3008–3013. - PubMed
-
- Herlitz J, Svensson L, Engdahl J, Silfverstolpe J. Characteristics and outcome I out of hospital cardiac arrest when patients are found in a non-shockable rhythm. Resuscitation. 2008;76:31–36. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
