

The role of pre-reduction MRI in the management of complex cervical spine fracture-dislocations: an ongoing controversy?
- PMID: 28904564
- PMCID: PMC5591568
- DOI: 10.1186/s13037-017-0139-8
The role of pre-reduction MRI in the management of complex cervical spine fracture-dislocations: an ongoing controversy?
Abstract
Background: Cervical spine fracture-dislocations in neurologically intact patients represent a surgical challenge due to the risk of inflicting iatrogenic spinal cord compression by closed reduction maneuvers. The use of MRI for early advanced imaging in these injuries remains controversially debated.
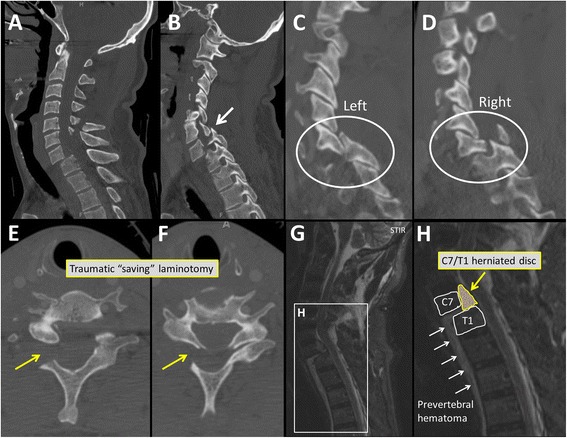
Case presentation: A 54-year old man sustained a fall over the handlebars of his racing bicycle. The helmeted patient sustained a fall on his head which resulted in a hyperflexion injury of the neck. He was neurologically intact on presentation. Initial CT imaging revealed a complex multisegmental cervical spine injury with a left-sided C6/C7 perched facet, a right sided C7/T1 fracture-dislocation, and a right-sided C6 and C7 traumatic laminotomy. The initial management consisted of temporary external Halo fixator application without closed reduction maneuver, to mitigate the risk of a delayed spinal cord injury. Subsequent advanced imaging by MRI revealed an acute traumatic C7/T1 disc herniation, with the intervertebral disc completely extruded into the spinal canal. Definitive surgical management was then accomplished by employing a three-stage anterior-posterior-anterior spinal decompression, realignment, fixation and fusion C4-T2 in one operative session. The patient recovered well and retained full neurological function. He resumed bicycle street racing within 10 months of the injury following successful spinal reconstruction.
Conclusions: The diagnostic evaluation of cervical fracture-dislocations should include advanced imaging by MRI in order to fully understand the injury pattern prior to proceeding with spinal reduction maneuvers which may impose the imminent threat of a devastating iatrogenic injury to the spinal cord. The presented staged management by initial Halo fixation without attempts for spinal reduction, followed by a surgical decompression and multilevel fusion, appears to represent a feasible and safe strategy for patients at risk of a delayed neurological injury.
Keywords: Cervical spine trauma; Fracture-dislocation; Intervertebral disc herniation; Patient safety; Perched facet; Spinal cord injury; Timing of surgery.
Conflict of interest statement
Ethics approval and consent for participation.
Written informed consent was obtained by the patient described in this article for publication of the content and the accompanying images shown in Figs. 1-4. The consent is available for review by the journal’s editor upon request. No ethical board approval was required for a case report.
Consent for publication.
Written informed consent was obtained by the patient described in this article for publication of the content and the accompanying images shown in Figs. 1-4. The consent is available for review by the journal’s editor upon request.
Competing interests
None of the authors declare a conflict of interest related to this article.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Kossmann T, Payne B, Stahel PF. Trentz O: [Traumatic paraplegia: surgical measures] Schweiz Med Wochenschr. 2000;130(22):816–828. - PubMed
-
- Kandziora F, Pflugmacher R, Scholz M, Schnake K, Putzier M, Khodadadyan-Klostermann C, Haas NP. Posterior stabilization of subaxial cervical spine trauma: indications and techniques. Injury. 2005;36(Suppl 2):B36–B43. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
