Rosette-forming Glioneuronal Tumor: A Rare Posterior Fossa Tumor in an Adolescent
- PMID: 28904578
- PMCID: PMC5588645
- DOI: 10.4103/jpn.JPN_12_17
Rosette-forming Glioneuronal Tumor: A Rare Posterior Fossa Tumor in an Adolescent
Abstract
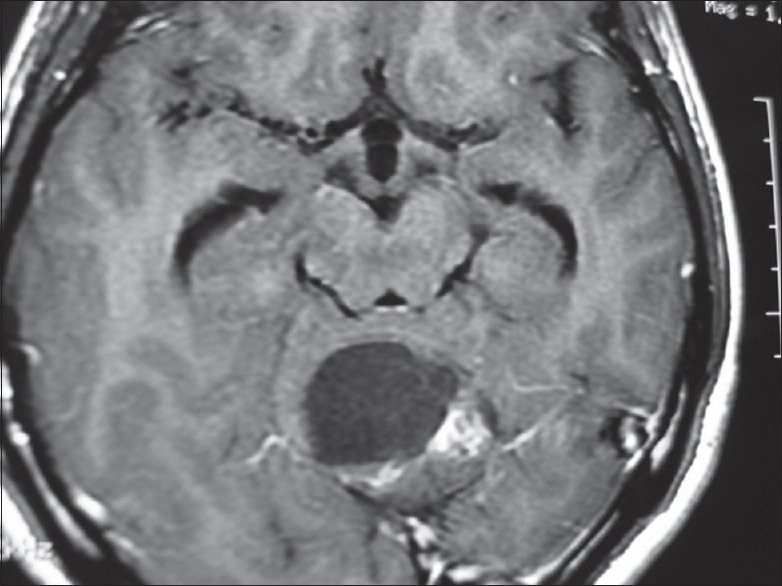
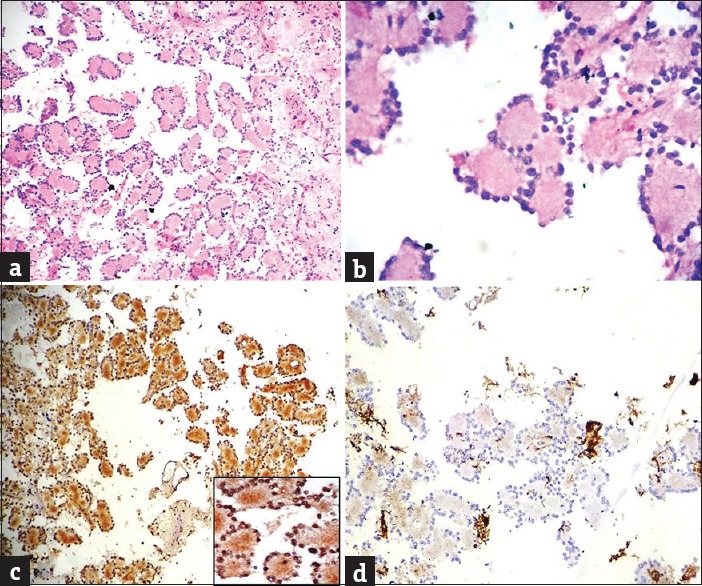
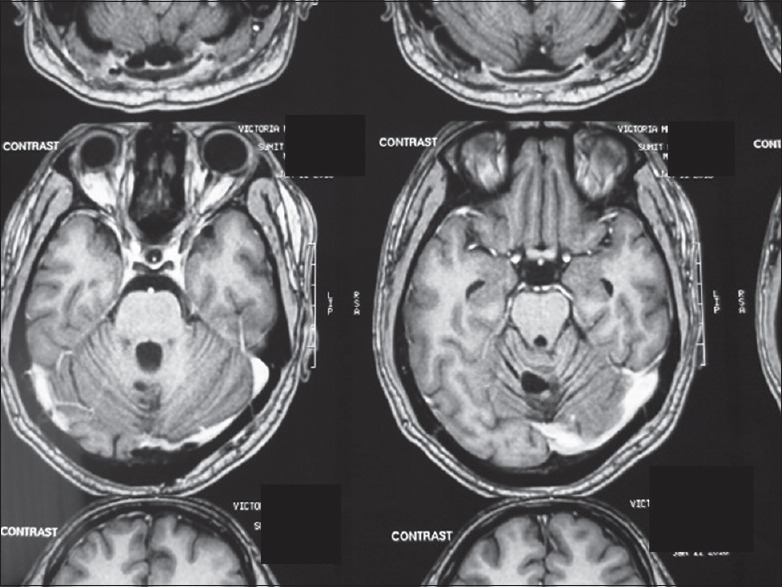
Rosette-forming glioneuronal tumor (RGNT) is a rare variety of slow growing mixed glioneuronal tumor involving primarily fourth ventricular region and occurring predominantly in young adults. We present a case of a 16-year-old boy who presented with dizziness and occipital headache. On radiological evaluation, a fairly large hypodense posterior fossa mass lesion in relation to the left side of the vermis, with a large cystic component was found. Surgical resection of the tumor was performed. Histopathological examination showed a biphasic tumor composed of bland neurocytic cells, arranged in the form of neurocytic rosettes along with glial areas resembling low-grade glioma. The neurocytic rich region shows strong synaptophysin positivity in the neuropil-rich core of the rosettes. Methylation-inhibited binding proliferative index was low (<1%). Based on these features, a diagnosis of RGNT was made. RGNT of the fourth ventricle should be considered in differential diagnosis of posterior fossa lesions, especially in relation to fourth ventricle and vermis in young adults.
Keywords: Adolescent; brain tumors; rosette-forming glioneuronal tumor.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Rosette-forming glioneuronal tumor of the fourth ventricle--case report.Neurol Med Chir (Tokyo). 2010;50(3):224-8. doi: 10.2176/nmc.50.224. Neurol Med Chir (Tokyo). 2010. PMID: 20339273
-
Rosette-forming glioneuronal tumour of the fourth ventricle: case report and review of the literature.Folia Neuropathol. 2016;54(1):80-7. doi: 10.5114/fn.2016.58919. Folia Neuropathol. 2016. PMID: 27179225 Review.
-
Coexpression of glial and neuronal markers in the neurocytic rosettes of rosette-forming glioneuronal tumors.Brain Tumor Pathol. 2014 Jan;31(1):17-22. doi: 10.1007/s10014-012-0133-x. Epub 2013 Jan 18. Brain Tumor Pathol. 2014. PMID: 23329202
-
Rosette-forming glioneuronal tumor of the fourth ventricle with advanced microvascular proliferation--a case report.Neuropathology. 2011 Aug;31(4):427-32. doi: 10.1111/j.1440-1789.2010.01168.x. Epub 2010 Nov 24. Neuropathology. 2011. PMID: 21092064
-
Rosette-Forming Glioneuronal Tumor Originating From the Spinal Cord: Report of 2 Cases and Literature Review.World Neurosurg. 2017 Feb;98:875.e1-875.e7. doi: 10.1016/j.wneu.2016.11.109. Epub 2016 Nov 30. World Neurosurg. 2017. PMID: 27915062 Review.
Cited by
-
Radiohistogenomics of pediatric low-grade neuroepithelial tumors.Neuroradiology. 2021 Aug;63(8):1185-1213. doi: 10.1007/s00234-021-02691-1. Epub 2021 Mar 29. Neuroradiology. 2021. PMID: 33779771 Free PMC article. Review.
-
Supratentorial intraventricular rosette-forming glioneuronal tumors - Case report and review of treatment paradigms.Surg Neurol Int. 2020 Jun 6;11:138. doi: 10.25259/SNI_188_2019. eCollection 2020. Surg Neurol Int. 2020. PMID: 32547825 Free PMC article.
-
Rosette-forming glioneuronal tumour of the fourth ventricle. Not always a foreseeable development.Contemp Oncol (Pozn). 2018;22(4):270-274. doi: 10.5114/wo.2018.81750. Epub 2018 Dec 31. Contemp Oncol (Pozn). 2018. PMID: 30783393 Free PMC article.
-
Rosette-forming glioneuronal tumor: an illustrative case and a systematic review.Neurooncol Adv. 2020 Sep 9;2(1):vdaa116. doi: 10.1093/noajnl/vdaa116. eCollection 2020 Jan-Dec. Neurooncol Adv. 2020. PMID: 33134925 Free PMC article. Review.
-
Malignant Transformation of a Rosette-Forming Glioneuronal Tumor with IDH1 Mutation: A Case Report and Literature Review.World Neurosurg X. 2019 Jan 5;2:100006. doi: 10.1016/j.wnsx.2018.100006. eCollection 2019 Apr. World Neurosurg X. 2019. PMID: 31218281 Free PMC article.
References
-
- Kuchelmeister K, Demirel T, Schlörer E, Bergmann M, Gullotta F. Dysembryoplastic neuroepithelial tumour of the cerebellum. Acta Neuropathol. 1995;89:385–90. - PubMed
-
- Komori T, Scheithauer BW, Hirose T. A rosette-forming glioneuronal tumor of the fourth ventricle: Infratentorial form of dysembryoplastic neuroepithelial tumor? Am J Surg Pathol. 2002;26:582–91. - PubMed
-
- Hainfellner JA, Scheithauer BW, Giangaspero F, Rosenblum MK. WHO Classification of Tumours of the Central Nervous System. 4th ed. Lyon: IARC Press; 2007. Rosette forming glioneuronal tumour of the fourth ventricle; pp. 115–6.
-
- Arai A, Sasayama T, Tamaki M, Sakagami Y, Enoki E, Ohbayashi C, et al. Rosette-forming glioneuronal tumor of the fourth ventricle – Case report. Neurol Med Chir (Tokyo) 2010;50:224–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources