

The efficacy of gabapentin in reducing pain intensity and postoperative nausea and vomiting following laparoscopic cholecystectomy: A meta-analysis
- PMID: 28906382
- PMCID: PMC5604651
- DOI: 10.1097/MD.0000000000008007
The efficacy of gabapentin in reducing pain intensity and postoperative nausea and vomiting following laparoscopic cholecystectomy: A meta-analysis
Abstract
Background: It is unknown whether gabapentin is effective in reducing acute pain following laparoscopic cholecystectomy. The purpose of the current meta-analysis was to evaluate the efficacy of gabapentin in reducing pain intensity and postoperative nausea and vomiting (PONV) after laparoscopic cholecystectomy.
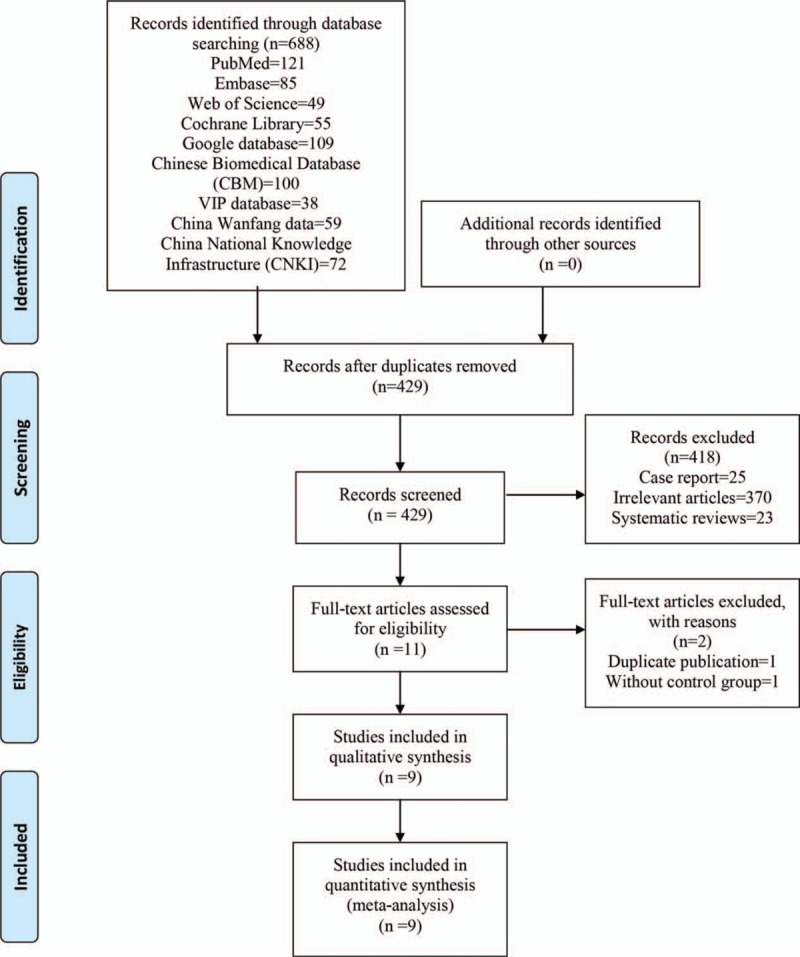
Methods: All randomized controlled trials (RCTs) evaluating the efficacy of gabapentin in reducing pain intensity and PONV after laparoscopic cholecystectomy were searched on the following databases: PubMed, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), the Google database, the Chinese Wanfang database, and the China National Knowledge Infrastructure (CNKI). The most recent literature search was conducted on March 21, 2017. Outcomes including visual analog scale (VAS) at 12 and 24 hours, total morphine consumption, and the occurrence of PONV. Continuous outcomes were expressed as the weighted mean difference (WMD) and 95% confidence interval (CI), and the one discontinuous outcome was expressed as risk ratio (RR) and 95% CI. Stata 12.0 software was used for meta-analysis.
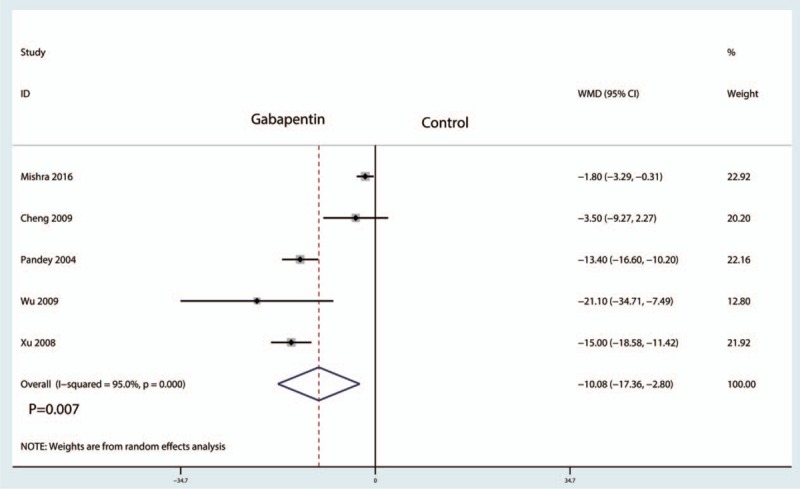
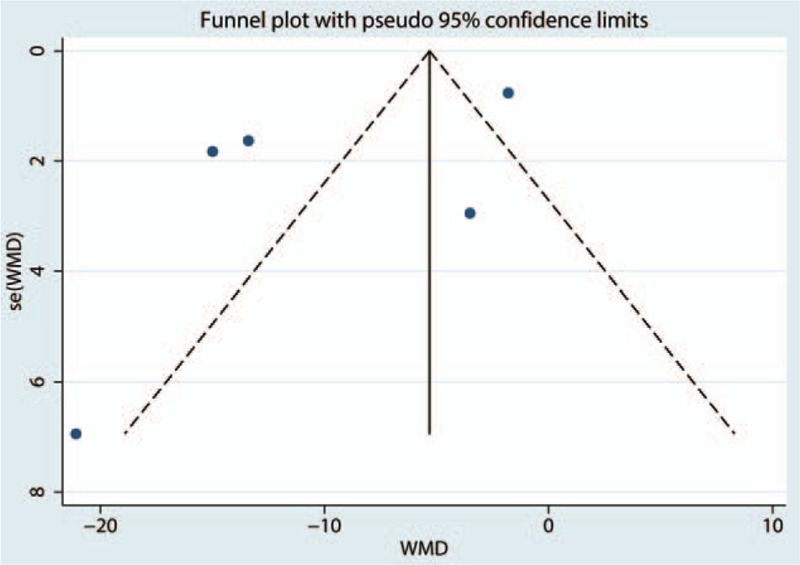
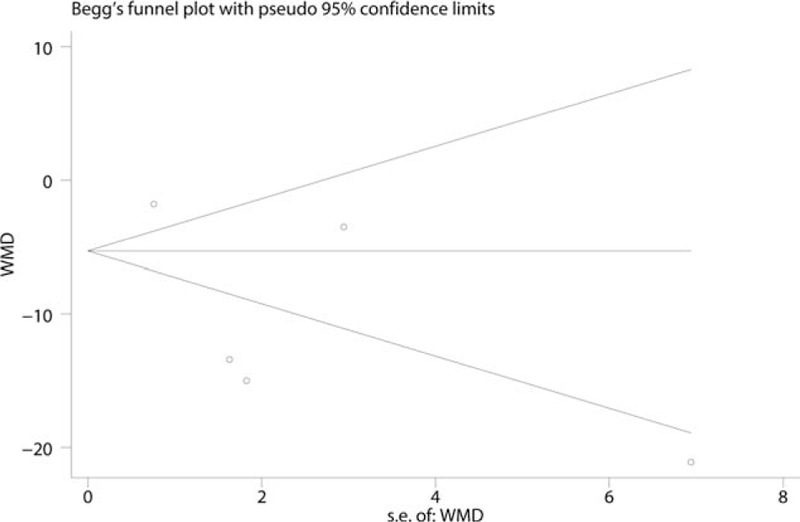
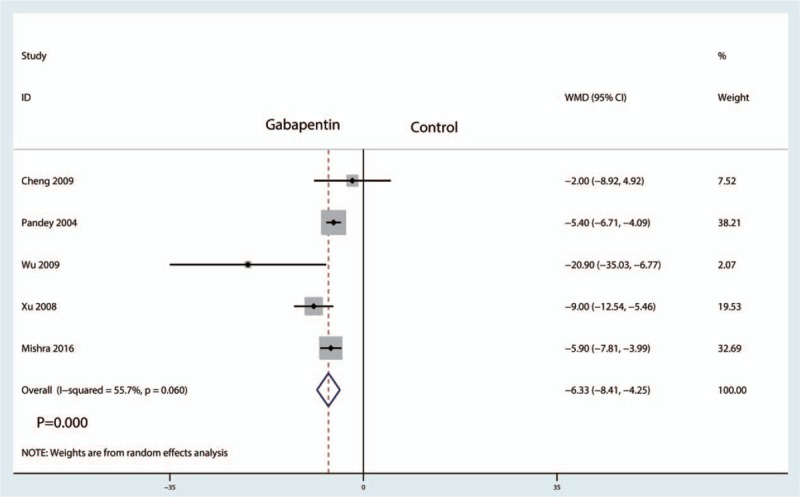
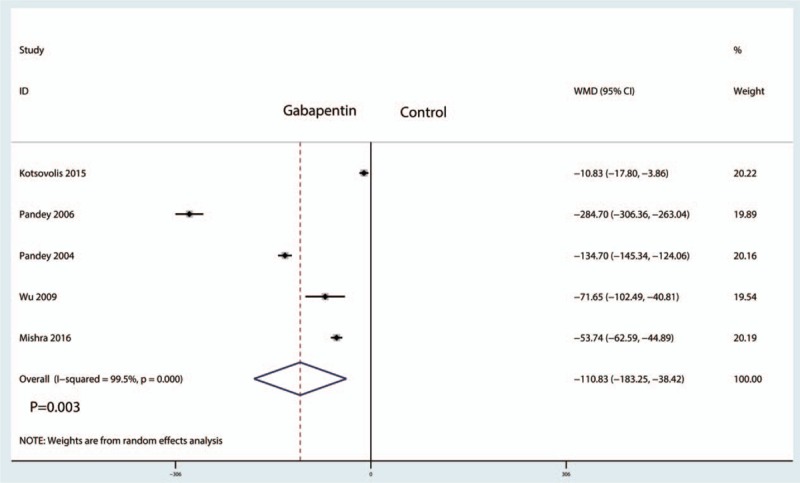
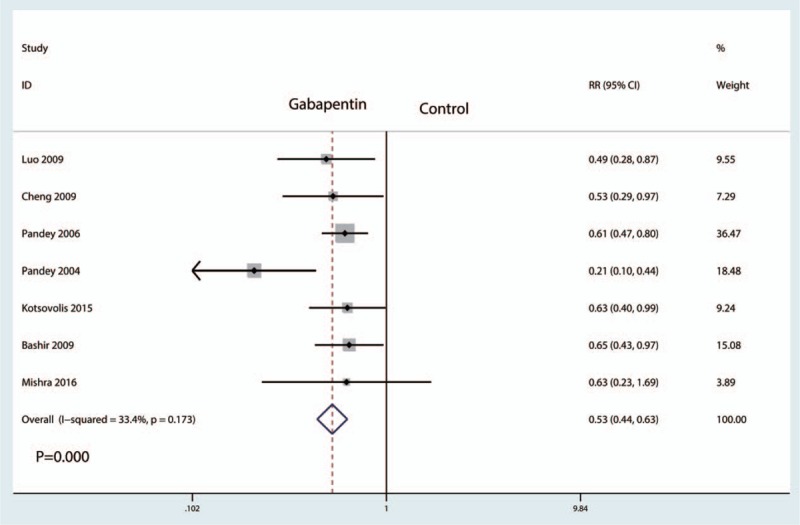
Results: A total of 9 studies involving 966 patients were identified. In total, there were 484 gabapentin subjects and 482 controls. Compared with the control group, gabapentin was associated with lower VAS at 12 hours (WMD = -10.18, 95% CI: -17.36 to -2.80, P = .007) and 24 hours (WMD = -6.33, 95% CI: -8.41 to -4.25, P = .000), which was equivalent on a 110-point VAS scale to 10.18 points at 12 hours and 6.33 points at 24 hours. Compared with the control group, gabapentin was associated with less total morphine consumption by approximately 110.83 mg (WMD = -110.83, 95% CI: -183.25 to -38.42, P = .003). In addition, the occurrence of nausea and vomiting in gabapentin was decreased (25.2% vs 47.6, RR = 0.53, 95% CI: 0.44-0.63, P = .000).
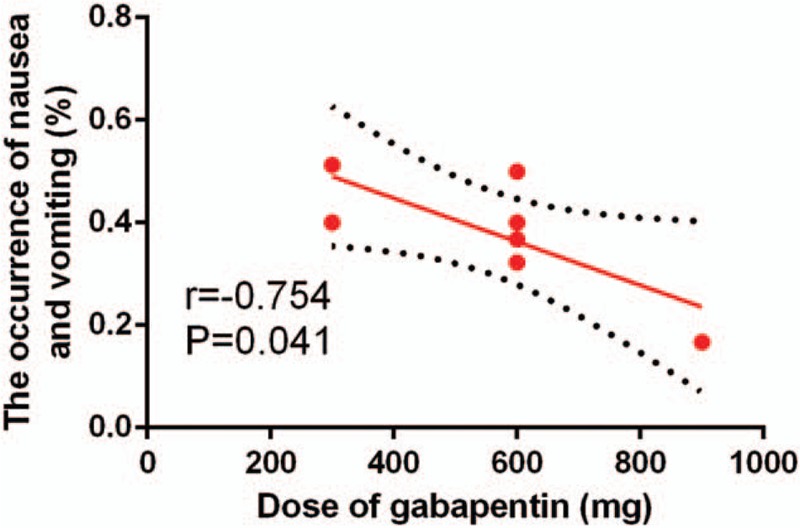
Conclusion: Gabapentin was efficacious in reducing postoperative pain, total morphine consumption, and morphine-related complications following laparoscopic cholecystectomy. In addition, there was a negative correlation between the gabapentin dosage and the occurrence of nausea and vomiting. The number of included studies is limited, and more studies are needed to verify the effects of gabapentin in laparoscopic cholecystectomy patients.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Naguib M, el Bakry AK, Khoshim MH, et al. Prophylactic antiemetic therapy with ondansetron, tropisetron, granisetron and metoclopramide in patients undergoing laparoscopic cholecystectomy: a randomized, double-blind comparison with placebo. Can J Anaesth 1996;43:226–31. - PubMed
-
- Pertusa V, Bellver J, Marques A, et al. [Antiemetic prophylaxis after laparoscopic cholecystectomy: comparative study of dehydrobenzperidol, metoclopramide, ondansetron and placebo]. Rev Esp Anestesiol Reanim 1996;43:239–42. - PubMed
-
- Fujii Y. The utility of antiemetics in the prevention and treatment of postoperative nausea and vomiting in patients scheduled for laparoscopic cholecystectomy. Curr Pharm Des 2005;11:3173–83. - PubMed
-
- Park IJ, Kim G, Ko G, et al. Does preoperative administration of gabapentin/pregabalin improve postoperative nasal surgery pain? Laryngoscope 2016;126:2232–41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
