

Comparison of fertility-sparing treatments in patients with early endometrial cancer and atypical complex hyperplasia: A meta-analysis and systematic review
- PMID: 28906392
- PMCID: PMC5604661
- DOI: 10.1097/MD.0000000000008034
Comparison of fertility-sparing treatments in patients with early endometrial cancer and atypical complex hyperplasia: A meta-analysis and systematic review
Abstract
Background: There are some fertility-sparing treatments in patients with early endometrial cancer (EEC) or atypical complex hyperplasia (ACH), and the objective is to compare them by evaluating the oncologic and reproductive outcomes.
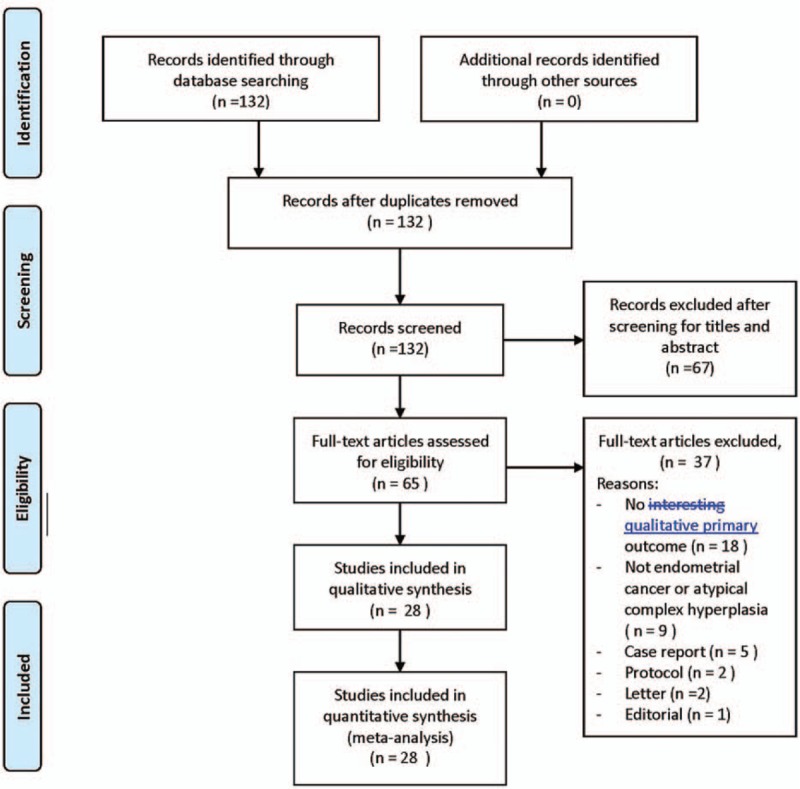
Methods: We searched the published literature using Medline, Cochrane, EMBASE, and Google Scholar databases up to January 3, 2017, with various combinations of keywords fertility-sparing treatments, progesterone, progestin, intrauterine devices, early endometrial cancer, and atypical complex hyperplasia. The primary endpoint is the complete response (CR) rate, and the secondary endpoints are the partial response (PR) rate, relapse rate (RR), pregnancy rate, and live birth rate.
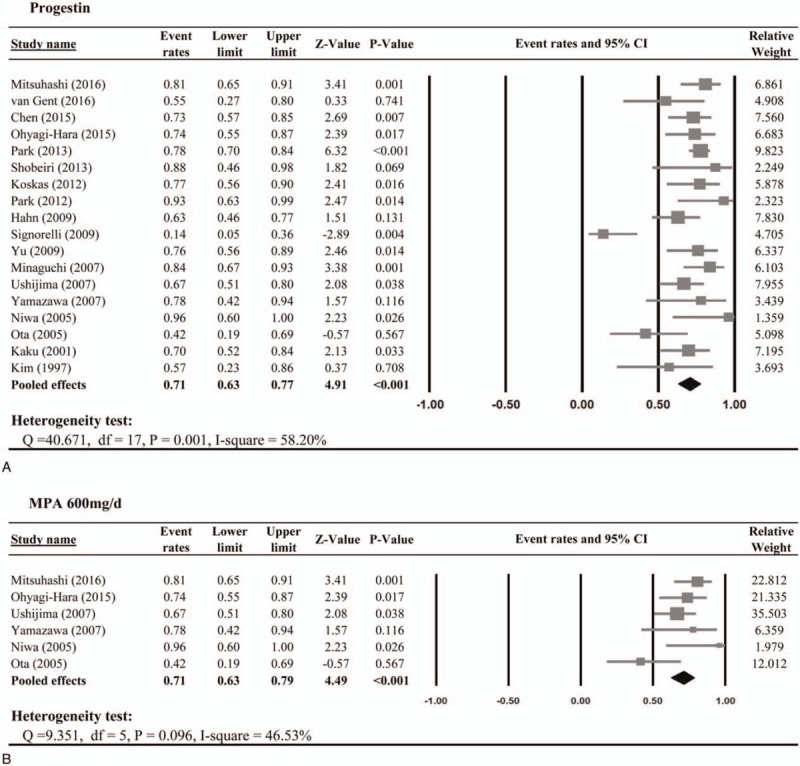
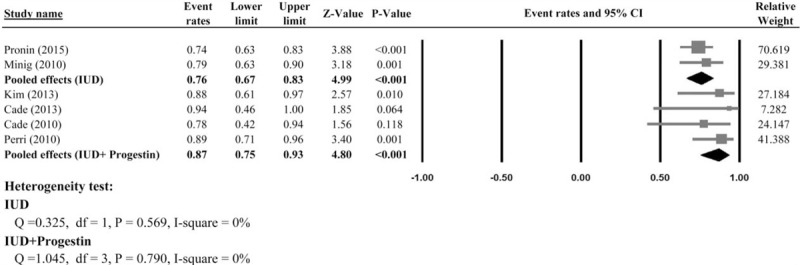
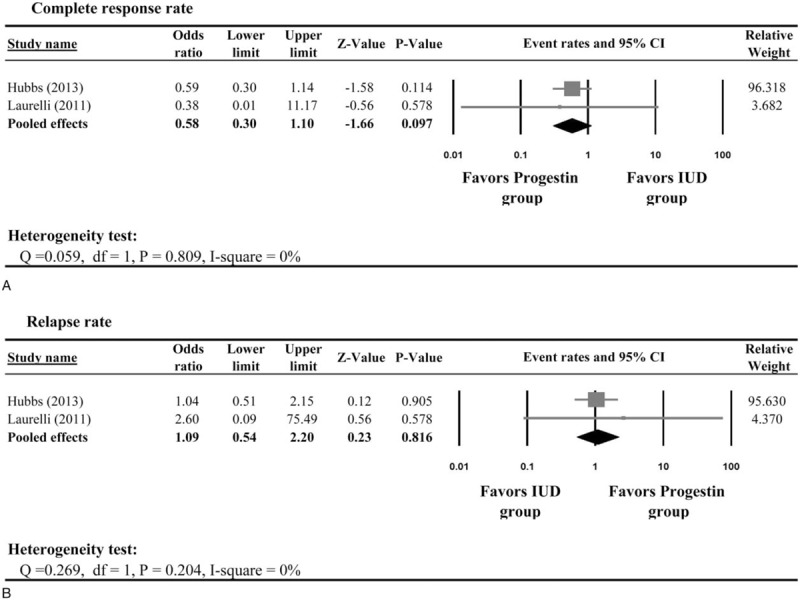
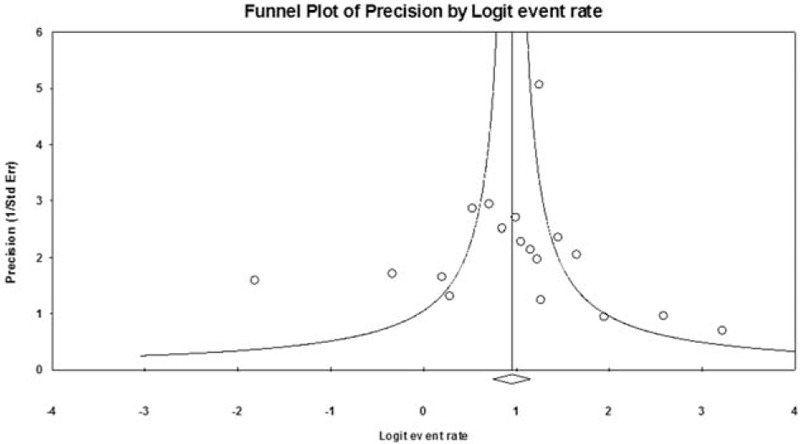
Results: Twenty-eight studies containing 1038 women with EEC or ACH were included for review and meta-analysis. The results demonstrated that women with EEC or ACH managed with progestin had a pooled CR rate of 71% (95% confidence interval [CI]: 63-77%). The pooled pregnancy outcomes showed that 34% of women taking progestin treatment for EEC or ACH became pregnant (95% CI: 30-38%); however, only 20% of them delivered live newborns. The pooled CR rate for women using intrauterine device (IUD) was 76% (95% CI: 67-83%), and pooled RR was 9% (95% CI: 5-17%). The pregnancy rate for women whom underwent IUD was 18% (95% CI: 7-37%), and 14% of them delivered live newborns. In patients using progestin plus IUD, the pooled CR rate was 87% (95% CI: 75-93%); among those patients, 40% became pregnant (95% CI: 20-63%), and 35% delivered live newborns. There is no publication bias for the CR rate.
Conclusion: For patients with EEC and ACH, treatments with progestin, with or without IUD, or IUD alone can reach good CR rate; however, the pregnancy outcomes might be worse in patients treated with IUD alone. Further randomized-controlled studies are warranted to find out a better solution.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2016;66:7–30. - PubMed
-
- Sherman ME. Theories of endometrial carcinogenesis: a multidisciplinary approach. Mod Pathol 2000;13:295–308. - PubMed
-
- Brownfoot FC, Hickey M, Ang WC, et al. Complex atypical hyperplasia of the endometrium: differences in outcome following conservative management of pre- and postmenopausal women. Reprod Sci 2014;21:1244–8. - PubMed
-
- Butterfield N, Smith JR. Role of imaging in fertility-sparing treatment of gynecologic malignancies. Radiographics 2016;36:2214–33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
