

Development of an integrated electronic platform for patient self-report and management of adverse events during cancer treatment
- PMID: 28911065
- PMCID: PMC5834137
- DOI: 10.1093/annonc/mdx317
Development of an integrated electronic platform for patient self-report and management of adverse events during cancer treatment
Abstract
Background: Significant adverse events (AE) during cancer therapy disrupt treatment and escalate to emergency admissions. Approaches to improve the timeliness and accuracy of AE reporting may improve safety and reduce health service costs. Reporting AE via patient reported outcomes (PROs), can improve clinician-patient communication and making data available to clinicians in 'real-time' using electronic PROs (ePROs) could potentially transform clinical practice by providing easily accessible records to guide treatment decisions. This manuscript describes the development of eRAPID (electronic patient self-Reporting of Adverse-events: Patient Information and aDvice) is a National Institute for Health Research-funded programme, a system for patients to self-report and manage AE online during and after cancer treatment.
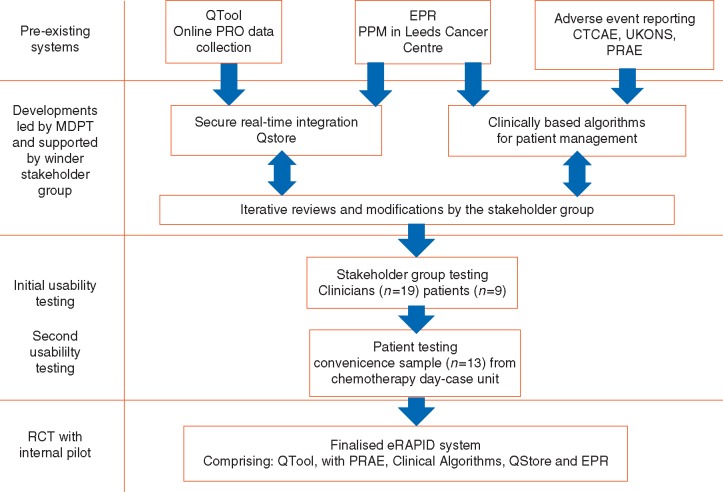
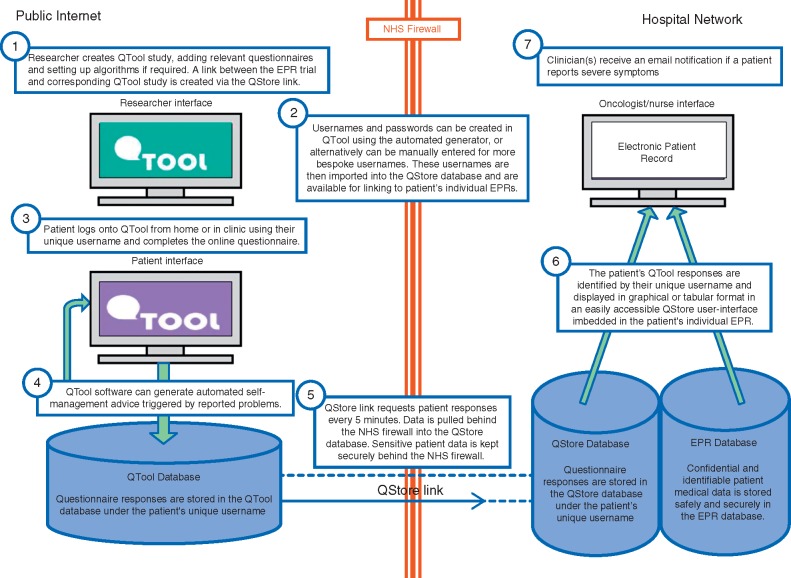
Materials and methods: A multidisciplinary team of IT experts, staff and patients developed using agile principles a secure web application interface (QStore) between an existing online questionnaire builder (QTool) displaying real-time ePRO data to clinicians in the electronic patient record at Leeds Teaching Hospitals NHS Trust. Hierarchical algorithms were developed corresponding to Common Terminology Criteria for Adverse Events grading using the QTool question dependency function. Patient advocates (N = 9), patients (N = 13), and staff (N = 19) usability tested the system reporting combinations of AE.
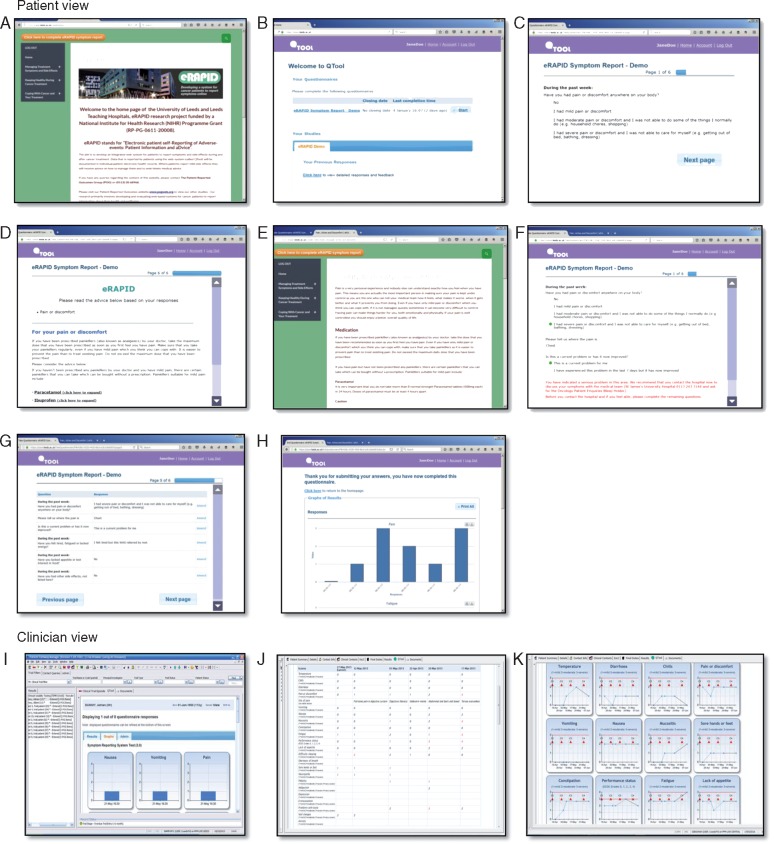
Results: The eRAPID system allows patients to report AE from home on PC, tablet or any web enabled device securely during treatment. The system generates immediate self-management advice for low or moderate AE and for severe AE advice to contact the hospital immediately. Clinicians can view patient AE data in the electronic patient record and receive email notifications when patients report severe AE.
Conclusions: Evaluation of the system in a randomised controlled trial in breast, gynaecological and colorectal cancer patients undergoing systemic therapy is currently underway. To adapt eRAPID for different treatment groups, pilot studies are being undertaken with patients receiving pelvic radiotherapy and upper gastrointestinal surgery. ISRCTN88520246.
Keywords: CTCAE; adverse events; electronic patient records; electronic patient-reported outcomes; integration; patient self-management.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Overcoming barriers to integrating patient-reported outcomes in clinical practice and electronic health records.Ann Oncol. 2017 Oct 1;28(10):2332-2333. doi: 10.1093/annonc/mdx506. Ann Oncol. 2017. PMID: 28961852 No abstract available.
References
-
- Mort D, Lansdown M, Smith N. et al. For Better, for Worse? A Review of the Care of Patients Who Died Within 30 Days of Receiving Systemic Anti-Cancer Therapy. London: National Confidential Enquiry into Patient Outcome and Death; 2008.
-
- De Luigi A. Analysis of reasons for admission to the emergency department for cancer patients. Ann Oncol 2002; 13: 112..
-
- Warrington L, Holch P, Kenyon L. et al. An audit of acute oncology services: Patient experiences of admission procedures and staff utilisation of a new telephone triage system. Support Care Cancer 24(12): 5041–5048. - PubMed
-
- Velikova G, Booth L, Smith AB. et al. Measuring quality of life in routine oncology practice improves communication and patient well-being: a randomized controlled trial. J Clin Oncol 2004; 22: 714–724. - PubMed
-
- Basch E, Bennett A, Pietanza MC.. Use of patient-reported outcomes to improve the predictive accuracy of clinician-reported adverse events. J Natl Cancer Inst 2011; 103: 1808–1810. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
