

Secondary malignant neoplasms, progression-free survival and overall survival in patients treated for Hodgkin lymphoma: a systematic review and meta-analysis of randomized clinical trials
- PMID: 28912173
- PMCID: PMC5622859
- DOI: 10.3324/haematol.2017.167478
Secondary malignant neoplasms, progression-free survival and overall survival in patients treated for Hodgkin lymphoma: a systematic review and meta-analysis of randomized clinical trials
Abstract
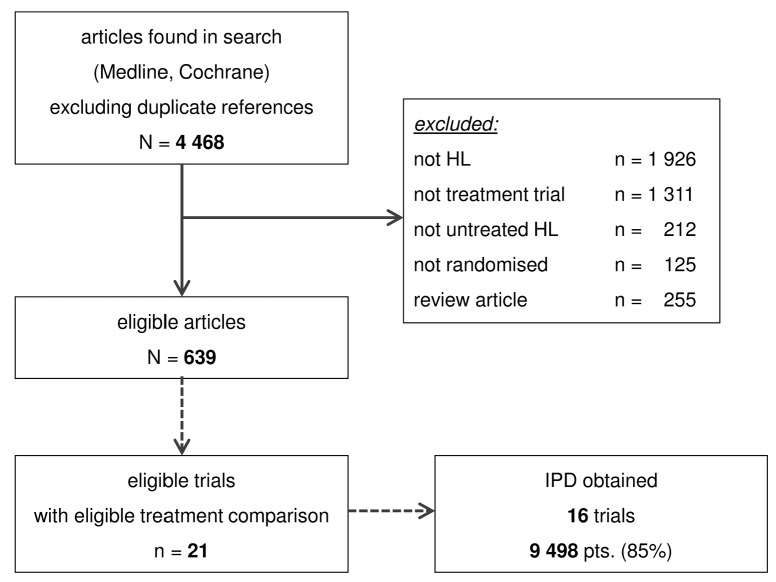
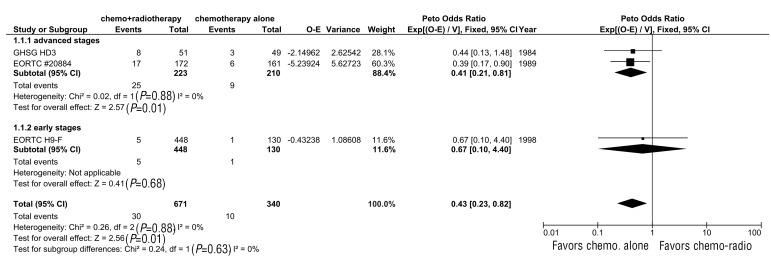
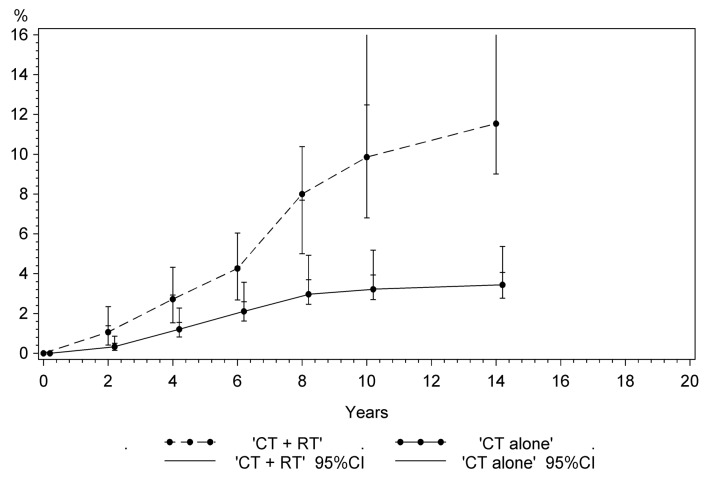
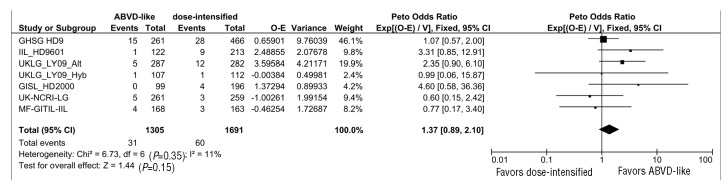
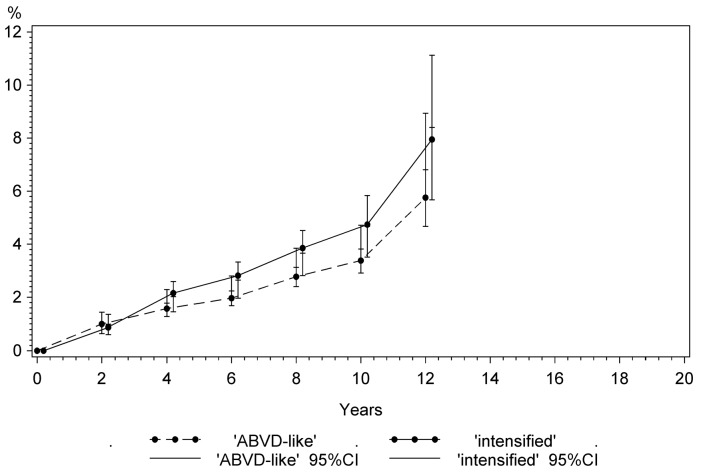
Treatment intensification to maximize disease control and reduced intensity approaches to minimize the risk of late sequelae have been evaluated in newly diagnosed Hodgkin lymphoma. The influence of these interventions on the risk of secondary malignant neoplasms, progression-free survival and overall survival is reported in the meta-analysis herein, based on individual patient data from 9498 patients treated within 16 randomized controlled trials for newly diagnosed Hodgkin lymphoma between 1984 and 2007. Secondary malignant neoplasms were meta-analyzed using Peto's method as time-to-event outcomes. For progression-free and overall survival, hazard ratios derived from each trial using Cox regression were combined by inverse-variance weighting. Five study questions (combined-modality treatment vs. chemotherapy alone; more extended vs. involved-field radiotherapy; radiation at higher doses vs. radiation at 20 Gy; more vs. fewer cycles of the same chemotherapy protocol; standard-dose chemotherapy vs. intensified chemotherapy) were investigated. After a median follow-up of 7.4 years, dose-intensified chemotherapy resulted in better progression-free survival rates (P=0.007) as compared with standard-dose chemotherapy, but was associated with an increased risk of therapy-related acute myeloid leukemia/myelodysplastic syndromes (P=0.0028). No progression-free or overall survival differences were observed between combined-modality treatment and chemotherapy alone, but more secondary malignant neoplasms were seen after combined-modality treatment (P=0.010). For the remaining three study questions, outcomes and secondary malignancy rates did not differ significantly between treatment strategies. The results of this meta-analysis help to weigh up efficacy and secondary malignancy risk for the choice of first-line treatment for Hodgkin lymphoma patients. However, final conclusions regarding secondary solid tumors require longer follow-up.
Copyright© 2017 Ferrata Storti Foundation.
Figures
References
-
- Eichenauer DA, Engert A, Andre M, et al. Hodgkin’s lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25 Suppl 3:iii70–75. - PubMed
-
- Borchmann P, Eichenauer DA, Engert A. State of the art in the treatment of Hodgkin lymphoma. Nat Rev Clin Oncol. 2012; 9(8):450–459. - PubMed
-
- Schaapveld M, Aleman BM, van Eggermond AM, et al. Second cancer risk up to 40 years after treatment for Hodgkin’s lymphoma. N Engl J Med. 2015; 373(26):2499–2511. - PubMed
-
- Swerdlow AJ, Higgins CD, Smith P, et al. Second cancer risk after chemotherapy for Hodgkin’s lymphoma: a collaborative British cohort study. J Clin Oncol. 2011; 29(31):4096–4104. - PubMed
-
- Aleman BM, van den Belt-Dusebout AW, De Bruin ML, et al. Late cardiotoxicity after treatment for Hodgkin lymphoma. Blood. 2007;109(5):1878–1886. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
