

Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy
- PMID: 28912181
- PMCID: PMC5654557
- DOI: 10.1161/CIRCRESAHA.117.311059
Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy
Abstract
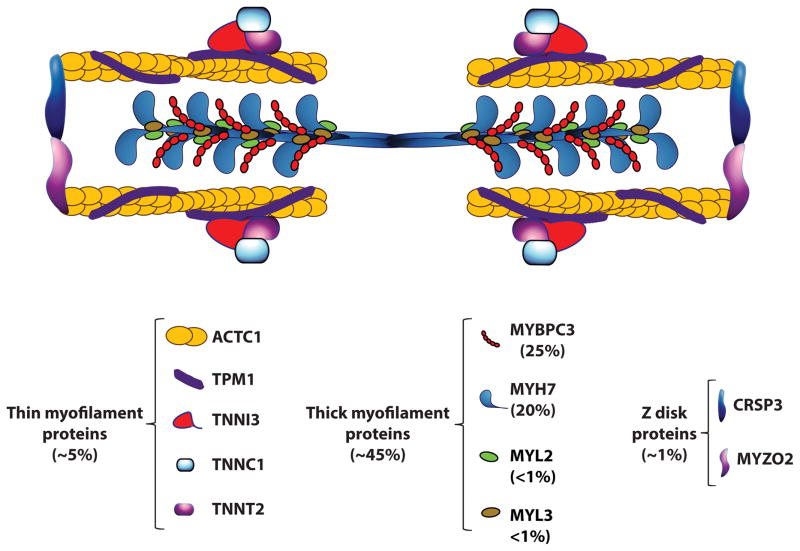
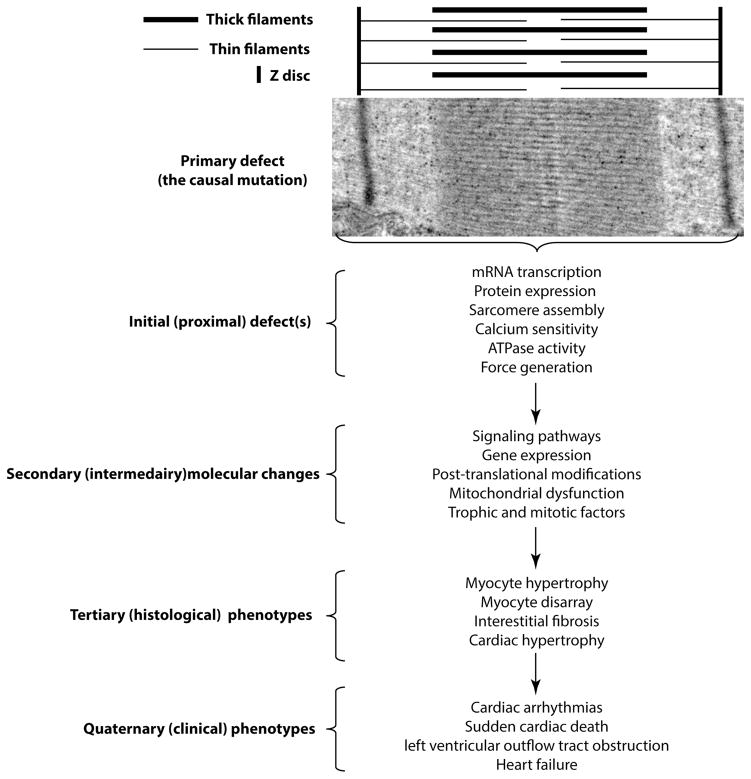
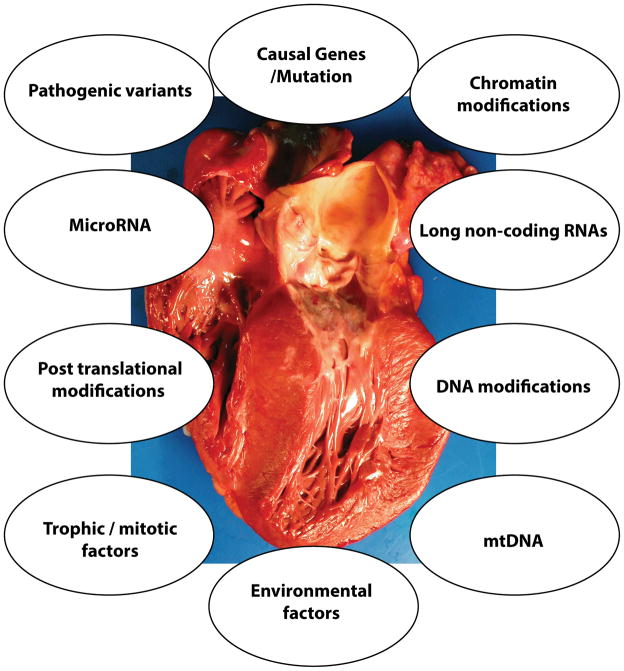
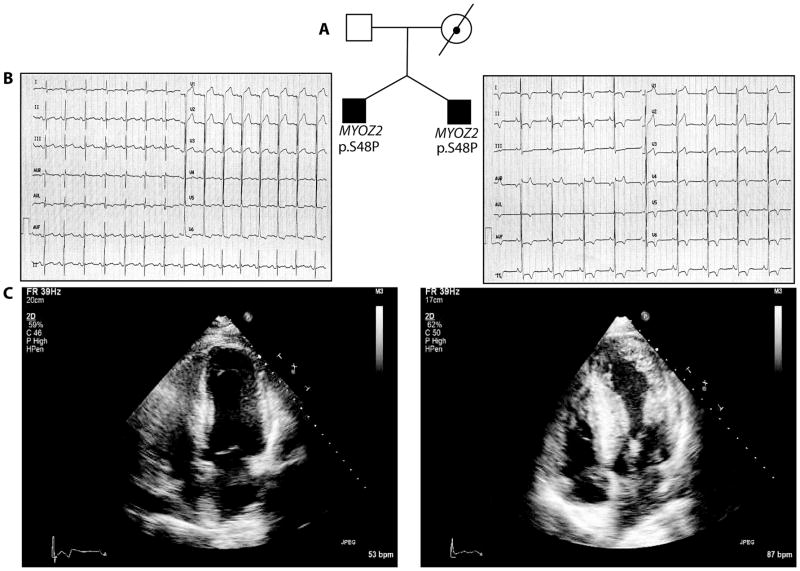
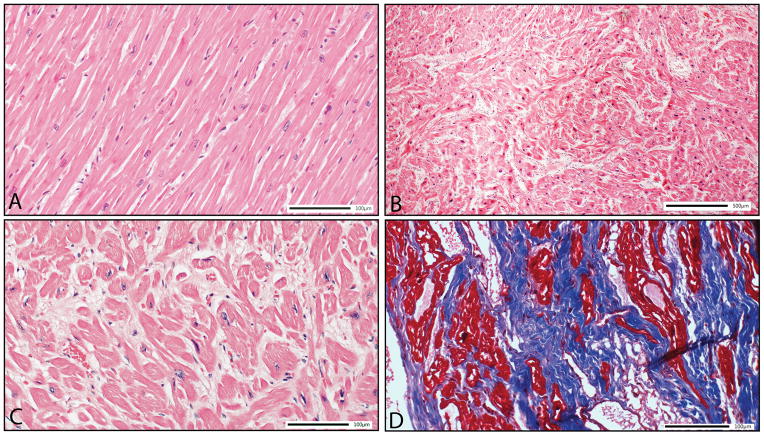
Hypertrophic cardiomyopathy (HCM) is a genetic disorder that is characterized by left ventricular hypertrophy unexplained by secondary causes and a nondilated left ventricle with preserved or increased ejection fraction. It is commonly asymmetrical with the most severe hypertrophy involving the basal interventricular septum. Left ventricular outflow tract obstruction is present at rest in about one third of the patients and can be provoked in another third. The histological features of HCM include myocyte hypertrophy and disarray, as well as interstitial fibrosis. The hypertrophy is also frequently associated with left ventricular diastolic dysfunction. In the majority of patients, HCM has a relatively benign course. However, HCM is also an important cause of sudden cardiac death, particularly in adolescents and young adults. Nonsustained ventricular tachycardia, syncope, a family history of sudden cardiac death, and severe cardiac hypertrophy are major risk factors for sudden cardiac death. This complication can usually be averted by implantation of a cardioverter-defibrillator in appropriate high-risk patients. Atrial fibrillation is also a common complication and is not well tolerated. Mutations in over a dozen genes encoding sarcomere-associated proteins cause HCM. MYH7 and MYBPC3, encoding β-myosin heavy chain and myosin-binding protein C, respectively, are the 2 most common genes involved, together accounting for ≈50% of the HCM families. In ≈40% of HCM patients, the causal genes remain to be identified. Mutations in genes responsible for storage diseases also cause a phenotype resembling HCM (genocopy or phenocopy). The routine applications of genetic testing and preclinical identification of family members represents an important advance. The genetic discoveries have enhanced understanding of the molecular pathogenesis of HCM and have stimulated efforts designed to identify new therapeutic agents.
Keywords: cardiomyopathy; cardiomyopathy, hypertrophic; death, sudden, cardiac; heart failure; human; mutation; myosin heavy chains.
© 2017 American Heart Association, Inc.
Figures

References
-
- Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the cardia study. Coronary artery risk development in (young) adults. Circulation. 1995;92:785–789. - PubMed
-
- Maron BJ, Mathenge R, Casey SA, Poliac LC, Longe TF. Clinical profile of hypertrophic cardiomyopathy identified de novo in rural communities. Journal of the American College of Cardiology. 1999;33:1590–1595. - PubMed
-
- Hada Y, Sakamoto T, Amano K, Yamaguchi T, Takenaka K, Takahashi H, Takikawa R, Hasegawa I, Takahashi T, Suzuki J, et al. Prevalence of hypertrophic cardiomyopathy in a population of adult japanese workers as detected by echocardiographic screening. The American journal of cardiology. 1987;59:183–184. - PubMed
-
- Zou Y, Song L, Wang Z, Ma A, Liu T, Gu H, Lu S, Wu P, Zhang dagger Y, Shen dagger L, Cai Y, Zhen double dagger Y, Liu Y, Hui R. Prevalence of idiopathic hypertrophic cardiomyopathy in china: A population-based echocardiographic analysis of 8080 adults. Am J Med. 2004;116:14–18. - PubMed
-
- Authors/Task Force m. Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, Mahrholdt H, McKenna WJ, Mogensen J, Nihoyannopoulos P, Nistri S, Pieper PG, Pieske B, Rapezzi C, Rutten FH, Tillmanns C, Watkins H. 2014 esc guidelines on diagnosis and management of hypertrophic cardiomyopathy: The task force for the diagnosis and management of hypertrophic cardiomyopathy of the european society of cardiology (esc) European heart journal. 2014;35:2733–2779. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
